


Introduction: The safety and efficacy of 1L dasatinib and 1L imatinib was established in the pivotal DASISION and IRIS trials; however, limited real-world evidence exists for the comparative effectiveness of these agents among US patients with CP-CML treated in routine clinical practice. As such, real-world data are needed to assess the outcomes of imatinib- and dasatinib-treated patients in a pragmatic setting. Additionally, recent data suggest that second generation tyrosine kinase inhibitors (TKIs), including dasatinib, may be beneficial in certain CP-CML populations, which may be underrepresented in clinical trials (e.g., high risk, elderly, or high body mass index [BMI]). This study examined the real-world clinical response rates and time to response associated with 1L dasatinib or 1L imatinib among patients with CP-CML, as well as in subgroups defined by Sokal risk, age, and BMI.
Methods: A retrospective, observational, US multi-site cohort study was conducted among adults with newly diagnosed Philadelphia chromosome-positive CP-CML treated with 1L dasatinib or 1L imatinib between January 2014 and September 2018. Patients had at least 1 year of follow-up after 1L initiation and did not have another malignancy or treatment as part of any clinical trial for CML. Oncologists collected data from eligible patient charts, including patient characteristics, treatment details, response to dasatinib or imatinib, and survival. Response was classified as major molecular response (MMR) and deep molecular response (DMR: 4.5-log reduction in BCR-ABL1 transcript levels) by physician report. Patient characteristics and outcomes were summarized using descriptive statistics for dasatinib and imatinib; results were reported in aggregate and stratified by Sokal risk (low and intermediate/high), age (< 65 and ≥ 65 years old), and BMI (low/normal [< 25 kg/m2] and high [≥ 25 kg/m2]). Comparisons were made by chi-square or Fisher's exact test for categorical variables, t-test or Wilcoxon test for continuous variables, log-rank test for overall survival (OS), and Cox proportional hazard models using Fine and Gray's method to account for competing risks in estimating differences in time to response across groups.
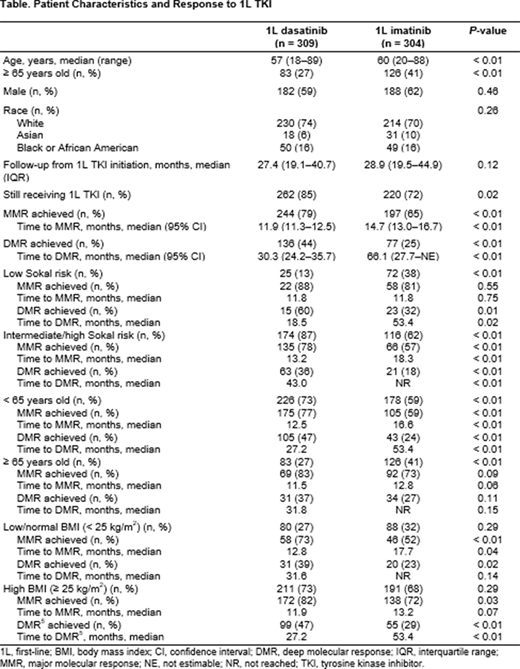
Results: Among the patients treated with 1L dasatinib (n = 309) and 1L imatinib (n = 304), median follow-up time was 27.4 and 28.9 months, respectively. Most patients initiated dasatinib at 100 mg (82%) or imatinib at 400 mg (95%). Dose reductions were more common among dasatinib patients vs imatinib (15% vs 7%, P < 0.01), though fewer dasatinib-treated patients discontinued for any reason (15% vs 28%, P < 0.01). Higher rates of MMR were seen in dasatinib vs imatinib patients (79% vs 65%, P < 0.01) and median time to MMR was shorter with dasatinib vs imatinib (11.9 vs 14.7 months, P < 0.01). Similarly, higher rates of DMR were seen among dasatinib vs imatinib patients (44% vs 25%, P < 0.01) along with a shorter median time to DMR with dasatinib vs imatinib (30.3 vs 66.1 months, P < 0.01). Among patients with intermediate/high Sokal risk, as well as those < 65 years old, rates of MMR and DMR were higher and achieved earlier with dasatinib vs imatinib (all P < 0.01) (Table). Low-risk patients treated with dasatinib had higher rates of DMR vs imatinib (60% vs 32%, P = 0.01). Among patients ≥ 65 years old, rates of MMR and DMR were numerically higher with dasatinib vs imatinib, though differences were not significant at α = 0.05. Across both BMI strata, rates of MMR and DMR were higher with 1L dasatinib vs 1L imatinib (all P < 0.05). In the overall population, dasatinib patients had superior OS compared to those treated with imatinib (98% vs 89%, P < 0.01).
Conclusions: In real-world clinical practice, a greater proportion of patients with CP-CML treated with 1L dasatinib achieved MMR and DMR and also achieved these responses earlier vs 1L imatinib. These clinically meaningful improvements were also observed across patient subgroups stratified by Sokal risk, age, and BMI. These findings from real-world US data were consistent with DASISION, demonstrating that dasatinib yields better outcomes among patients with CP-CML, with the novel findings of improved OS and improved outcomes in certain subgroups, including a higher rate of DMR among low-risk patients.
Klink:Cardinal Health: Current Employment, Current equity holder in publicly-traded company. Keating:Bristol Myers Squibb: Current Employment. Brokars:Bristol Myers Squibb: Current Employment. Kee:Bristol Myers Squibb: Current Employment. Copher:Bristol Myers Squibb: Current Employment. Stwalley:Bristol Myers Squibb: Current Employment, Current equity holder in publicly-traded company. Feinberg:Cardinal Health: Current Employment. Jabbour:Takeda: Other: Advisory role, Research Funding; AbbVie: Other: Advisory role, Research Funding; Genentech: Other: Advisory role, Research Funding; Amgen: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding; BMS: Other: Advisory role, Research Funding.
This icon denotes a clinically relevant abstract

