Background: Immune thrombocytopenia (ITP) is an autoimmune disorder characterized by isolated thrombocytopenia. Splenectomy remains an effective and safe treatment for ITP.
Objective: Identify and estimate risk factors associated with no response (platelet count < 30 x 109/L) to splenectomy for adult ITP patients.
Patients and Methods: The study conducted at National Research Center for Hematology (Moscow) from 03/2015 to 11/2019 included all patients (in total, 111) with ITP, who underwent laparoscopic splenectomy. Median (Med) platelet count at admission was 12 x 109/L (range from 1 to 239 x 109/L). The time from diagnosis of ITP to splenectomy varied from 3 months to 51 years. All patients had received from 1 to 3 lines of treatment prior to splenectomy. Pre-splenectomy treatment was carried out at platelet count < 20 x 109/L and/or in the presence of bleeding.
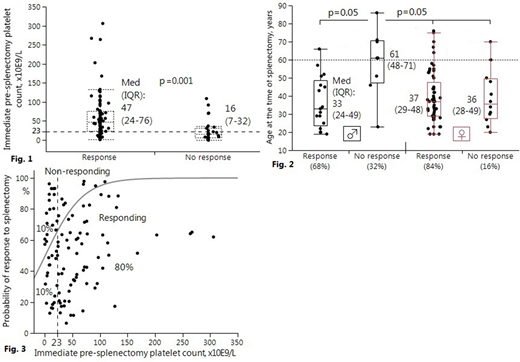
Results: Of the 111 patients 31 were male (Med age 43 years [IQR 27-55]) and 80 were female (Med age 37 [IQR 29-49]). The male/female ratio was 1:2.6. Complete response to splenectomy (platelet count > 100 x 109/L) was achieved in 79/111 (71.2%) cases, 11/111 (9.9%) patients had partial response (platelet count: 30-100 x 109/L) and 21/111 (18.9%) failed to respond (platelet count < 30 x 109/L). Patients who achieved complete response to splenectomy had a significantly higher immediate pre-splenectomy platelet count than non-responders: Med platelet count (95% CI): 47 (35-58) vs 16 (9-20) (x 109/L), Mann-Whitney U test, P < 0.001 (CI, confidence interval) (Figure 1). Multivariate logistic regression analysis was carried out to identify factors associated with splenectomy outcome (response/no response). Multivariate analysis included patient's gender and age, duration of ITP, grade of bleeding at admission, platelet count at admission, preoperative platelet count and number of prior lines of therapy. Continuous variables were dichotomized using ROC analysis, in particular, cut-off point for preoperative platelet count was 23 x 109/L. As a result, following statistically significant (Wald test) factors were selected:
• an unfavorable predictor: immediate pre-splenectomy platelet count < 23 x 109/L, RR (95% CI): 2.5 (1.1-8.6), P = 0.001 (RR, relative risk) (Figure 1) and
• combined unfavorable risk factor: male gender in the age over 60 (compared to men in the age ≤60 and women in general), RR (95% CI): 2.0 (0.9-7.1), P = 0.05 (Figure 2).
Response rate was negatively correlated (in univariate analysis) with the number of treatment lines prior to splenectomy (negative Spearman's rank correlation coefficient, −0.30; P = 0.01). When preoperative platelet count ≥ 23 x 109/L was achieved, probability of complete response to splenectomy was 80% (Figure 3). The rate of postoperative complications was 12.6%. According to our follow-up data (up to 5 years) 66/79 (83.5%) patients maintained complete response.
Conclusions: High-risk groups were identified: patients with immediate pre-splenectomy platelet count < 23 x 109/L (i.e. with no effect of preoperative treatment) and men over the age of 60. Identified risk factors could be taken into account in decision-making process.
No relevant conflicts of interest to declare.