

Background: Follicular lymphoma (FL) commonly recurs and is difficult to cure. Obinutuzumab (OBI) is a humanized type II anti-CD20 antibody. It's mode of action is mainly characterized by the induction of direct cell death and it shows stronger antibody-dependent cellular cytotoxicity (ADCC) than rituximab. While OBI is indicated for previously untreated or relapsed/refractory (r/r) FL, there is no evidence on the efficacy of retreatment with OBI in r/r FL after prior OBI-containing therapy. To demonstrate the effectiveness of OBI-retreatment in a non-clinical study, we established in vitro and in vivo OBI resistant models, consisting of human non-Hodgkin lymphoma (NHL) cells resistant to OBI-induced ADCC and OBI-resistant tumors established from NHL cells under xenotransplantation conditions, and investigated the combination efficacy of OBI and bendamustine (Benda) in these OBI-resistant models.
Methods: OBI-induced ADCC resistant clones were established from an RL cell line by inducing ADCC three times with CD16-transfected NK-92 cells. The in vivo resistant model was established from a SU-DHL-4 xenograft model through repeated treatment with OBI and re-inoculation of the regrown tumors. CD20 expression was assessed by flow cytometry or immunohistochemistry (IHC). ADCC activity was evaluated using calcein-AM with CD16-transfected NK-92 cells. To examine antitumor activity, OBI, human immunoglobulin G (HuIgG), Benda, or vehicle were intravenously administered on Day 1, 8 and 15 (OBI and HuIgG) or Day 1 and 2 (Benda and vehicle), and tumor volume was measured. Intratumorally infiltrated NK cells were assessed by IHC of CD335. Cell surface CD107a expression was assessed by flow cytometry.
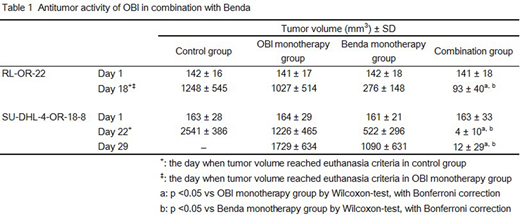
Results: OBI-induced ADCC resistant clones derived from RL (RL-OR-8 and RL-OR-22) showed a reduction in ADCC sensitivity compared with RL. These resistant clones exhibited CD20 expression similar to RL. Pretreatment of the effector NK cells with Benda enhanced ADCC induction of OBI in RL-OR-8 and RL-OR-22. Treatment with OBI (30 mg/kg) in combination with Benda (13.3 mg/kg) also significantly increased antitumor activity compared with each single agent alone on Day 18 (when tumor volume reached euthanasia criteria (*) in control and OBI monotherapy groups) in the RL-OR-22 xenograft model (Table 1). An in vivo OBI resistant model derived from SU-DHL-4 xenografts (SU-DHL-4-OR-18-8) was also established. While SU-DHL-4 xenografted tumors disappeared in 6/6 mice after the third OBI treatment (6 mg/kg), SU-DHL-4-OR-18-8 tumors did not regress in 6/6 mice. CD20 expression in SU-DHL-4-OR-18-8 tumors did not decrease compared with SU-DHL-4 tumors. The ratio of CD335-positive cells to tumor cells after 6 mg/kg of OBI treatment (Day 4) in SU-DHL-4-OR-18-8 was significantly decreased compared with the ratio in SU-DHL-4 (0.31 ± 0.12% vs 0.93 ± 0.23%). The combination efficacy of OBI and Benda was also assessed in an SU-DHL-4-OR-18-8 xenograft model. OBI (6 mg/kg) in combination with Benda (25 mg/kg) significantly increased the antitumor activity compared with each single agent alone on Day 22 (*in control group) and 29 (Table 1). Finally, the expression of CD107a, an NK cell-degranulation marker, was detected to examine the effect of Benda on NK activity in vitro. Pretreating effector NK cells with Benda upregulated CD107a expression on NK cell surfaces after OBI treatment in RL-OR-8 and RL-OR-22.
Conclusions: The decreased CD335-positive cell ratio observed in the in vivo SU-DHL-4-OR-18-8 resistant model suggests that the mechanism of resistance to OBI also involves the attenuation of ADCC as in the in vitro OBI-induced ADCC resistant clones. The combination treatment of OBI and Benda was effective in both RL-OR-22 and SU-DHL-4-OR-18-8 xenograft models. It is possible that activation of NK cells by Benda might be involved in this combination mechanism. Although the mechanisms need to be examined in more detail, these results indicate the possible effectiveness of OBI-retreatment after prior OBI-containing therapy.
Yamashita-Kashima:Nippon Shinyaku Co., Ltd.: Research Funding; Chugai Pharmaceutical Co., Ltd.: Current Employment. Kawasaki:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Yorozu:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Yoshiura:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Fujimura:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Kurasawa:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Harada:Chugai Pharmaceutical Co., Ltd.: Current Employment; Nippon Shinyaku Co., Ltd.: Research Funding. Yoshimura:Nippon Shinyaku Co., Ltd.: Research Funding; Chugai Pharmaceutical Co., Ltd.: Current Employment.

