


INTRODUCTION:
The serotonin release assay (SRA) is considered the gold standard for diagnosis of heparin-induced thrombocytopenia (HIT). While the SRA holds high sensitivity and specificity when results are definitive, up to 10% of samples from patients with suspected HIT yield "indeterminate" results. In classic HIT, the SRA typically reveals high levels of serotonin release when serum is mixed with low concentrations of heparin and low levels of serotonin release when serum is mixed with high concentrations of heparin. Results are considered "indeterminate" when high levels of serotonin release are seen at both low and high concentrations of heparin, indicating a failure of high-dose heparin to saturate the heparin binding sites of PF4 molecules and inhibit platelet activation. Explanations for indeterminate assays include the presence of heparin-binding proteins that interfere with the assay, high titers of HLA class I alloantibodies, or immune complexes. Since the diagnosis of HIT carries such significance and has so many ramifications, an indeterminate SRA may leave therapeutic indecision. The etiologies, platelet trends, clinical course and outcomes of patients that receive indeterminate SRA results are not well-understood. We conducted a retrospective review of 2,056 patients that underwent SRA testing as part of their evaluation for HIT.
METHODS:
Using the electronic medical record data extraction software Clinical Looking Glass, we identified patients that underwent SRA testing between 1/1/2014 and 12/31/2018. SRA results were considered "indeterminate" when serotonin release exceeded 19% at all heparin dilutions (0.1 U/mL, 0.5 U/mL and 10 U/mL). We conducted a retrospective chart review to study the clinical course among patients who had "indeterminate" SRA results, the trends in platelet count, the timing of platelet drops and the physician response to this result. Statistical analysis was performed using chi-square testing for categorical variables.
RESULTS:
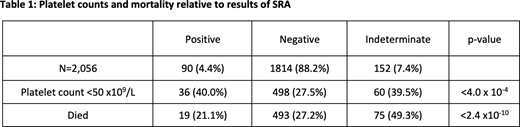
We identified 2,056 patients that underwent SRA testing between 2014 and 2019. Of these, 90 patients (4.4%) had "positive" SRA results and 1,814 patients (88.2%) had "negative" SRA results. Among the 152 patients (7.4%) with "indeterminate" SRA results, the mean 4T score was just 2.9, corresponding to a HIT probability of <5%. One-hundred and twenty of these 152 patients (78.9%) had heparin-PF4 antibody testing with optical densities below 0.60 OD, while only 4 of 152 patients (2.6%) had optical densities above 2.00 OD. Seventy eight of 152 patients (51.3%) either continued or were re-exposed to heparin after the indeterminate SRA result, and in 71 of 78 cases (91.0%), the platelet count stabilized or improved despite heparin exposure. In the remaining 7 cases, no acute VTE were found and no diagnosis of HIT was made. Four of the 71 patients (5.6%) that continued or were re-exposed to heparin were noted to have an acute VTE.
A significantly higher portion of patients with an indeterminate SRA died during admission compared to those with a positive or negative SRA (49.3% vs. 21.1% and 27.2%, p <2.4 x10-10). The prevalence of thrombocytopenia <50,000 was substantially higher in patients with an indeterminate or positive SRA, compared to those with a negative SRA (39.5% and 40.0% vs. 27.5%, p <4.0 x 10-4). Re-exposure or continuation of heparin did not affect mortality; patients that were given heparin after an indeterminate SRA had a 47.4% mortality, compared to 51.4% in those given no more heparin (p = 0.63). Table 1 summarizes these findings.
CONCLUSIONS:
This is the largest study to date looking at patients with indeterminate SRA testing results, in which platelets exhibit high levels of serotonin release at both low and high heparin concentrations. Our data suggest 1) the majority of patients with indeterminate SRAs likely did not have HIT, 2) as evidenced by the low 4T scores and heparin-PF4 antibody levels, an indeterminate SRA suggests thrombocytopenia related to in-vivo platelet activation, and 3) an indeterminate SRA is associated with increased mortality.
SRA results warrant a case-by-case assessment of the clinical picture in order to avoid unnecessary cessation of heparin products. Further studies exploring the mechanism leading to high serotonin release at both low and high heparin concentrations, causing an "indeterminate" SRA result, are warranted.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

