

Background: Polycythemia vera (PV), Essential Thrombocytosis (ET) and Primary Myelofibrosis (PMF) are Myeloproliferative Neoplasms (MPNs) with median age at diagnosis of ~56-70 years old. However, around 10%-15% of cases are diagnosed during young adulthood and there are scanty data about their molecular profile and its implications in clinical outcomes.
Objective: To analyze the clinical and molecular characteristics of young adult patients (≤45y.o.) with MPNs (Y-MPN) and to correlate them with clinical features and outcomes.
Material and Methods: This is a retrospective single-center study including MPN patients diagnosed below the age of 45 years. Molecular characterization was performed using DNA from granulocytes at diagnosis or before the start of cytoreductive therapy. JAK2V617F was assessed by quantitative allele-specific PCR and CALR mutations by fragment analysis of exon 9. Further molecular profiling was performed by next generation sequencing (NGS) with a custom panel of 25 myeloid-associated genes (ASXL1, CALR, CBL, CSF3R, DNMT3A, ETV6, EZH2, IDH1, IDH2, JAK2, KIT, KRAS, MPL, NRAS, PRPF8, RUNX1, SETPB1, SF3B1, S2HB3, SRSF2, STAG2, TET2, TP53, U2AF1 and ZRSR2) using Illumina technology. Pathogenic mutations in genes previously related with poor outcomes (ASXL1, EZH2, IDH1, IDH2, SRSF2 and U2AF1) were named as Mutations of Adverse Significance (MAS). Molecular alterations were correlated with diagnosis, progression to PV post ET (PVpET), progression to MF post PV/ET (MFpPV/ET), start of cytoreduction and major thrombotic events (MTE). Time to progression (TTP) and overall survival (OS) were calculated from diagnosis to progression (ELN criteria) and to last visit.
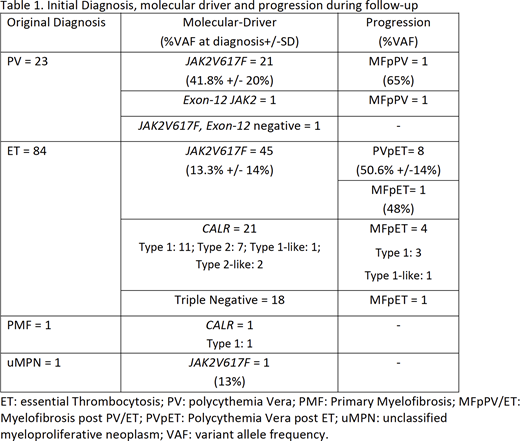
Results: From 646 MPN followed in our clinic, 109 (17%) cases were Y-MPN; females 72 (66.1%). At diagnosis the median age was 35 y.o. (9-45). 23 patients (21%) were PV, 91% carried JAK2V617F, 4% (1) carried an exon-12 JAK2 mutation and 1 was JAK2V617F and exon-12 negative. 84 cases (77.1%) were ET, 53.5% (45) JAK2V617F, 25% (21) CALR, (52% type-1 mutation, see table) and 21.4% (18) triple negative (TN). There was 1 PMF with CALR type-1 mutation. No MPL canonical mutations were found. ET was predominantly diagnosed in females (M/F: 26/58). Regarding clinical variables, we found a high proportion of ET-JAK2V617F with high LDH values, higher platelet count for CALR-ET and ET-TN patients (967 and 978 vs 728 for ET-JAK2V617F, p=0.03) and higher frequency of MTE at or before diagnosis for JAKV617F cases (p=0.001). The mean follow-up was 152 months (SD +/-10.4); 16 progressions were registered (PFS 305 months); 8 patients to MFpPV/ET and 8 ET-JAK2V617F to PVpET. An increase in the VAF of JAK2V617F was observed at the time of progression either to PVpET or to MFpET/PV (see table). Seven MTE were registered during this time, 3 in JAK2V617F, 2 in CALR type-1, 1 in exon-12 and 1 in a TN case. 38 (34.8%) cases started cytoreduction, with median time to cytoreductive therapy of 251 (172-330) months; JAK2V617F cases started cytoreduction more often (p=0.04) than patients with other genotypes. No progression to AML nor deaths were recorded.
The NGS panel was performed in 102 (93.5%) cases. Pathogenic mutations in non-driver genes were found in 41.2% (42) of cases, being TET2 (7%), ASXL1 (6%) and DNMT3A (5%) the most frequently mutated genes. Also, in 28.4% (29) variants of unknown significance (VUS) were found, involving TET2 (6%), SETBP1 (4%), SH2B3 (5%), and JAK2 (4%) among others. The mutations in SH2B3 (1 pathogenic, 5 VUS) were more frequent in JAK2V617F patients and those in DNMT3A were more common in PV patients. The presence of mutations in non-driver genes (pathogenic or VUS) did not correlate with MTE before or after diagnosis, the start of cytoreduction nor clonal progression. Regarding the 19 TN cases, in 7 (36.8%) one or more non-canonical pathogenic variants implicating MPL, JAK2 and TET2 genes were found. Finally, 8 patients (7.8%) harbored a MAS, of which 3 progressed to MF (2 CALR to MF and 1 ET-JAK2V617F to PVpET); TTP was similar to the rest of the cohort.
Conclusions: Our data show that 41% of Y-MPN patients harbor pathogenic mutations in non-driver genes. There was no correlation between their presence and clonal progression, major thrombotic events or overall survival. Mutations of adverse significance did not predict major clinical outcomes. Monitoring of JAK2V617F allele-burden can help to predict progression to MFpPV/ET or PVpET.
Andrade-Campos:Sanofi-Genzyme: Consultancy, Speakers Bureau; Takeda-Shire: Speakers Bureau; Celgene-BMS: Consultancy. Fernández:Roche: Consultancy, Speakers Bureau. Salar:Janssen: Speakers Bureau; Roche: Speakers Bureau; Celgene: Speakers Bureau. Bellosillo:Qiagen: Consultancy, Speakers Bureau; Roche: Consultancy, Research Funding, Speakers Bureau.

