


Introduction:
Immune thrombocytopenia (ITP) is a hematological disease associated with thrombocytopenia and bleeding diathesis. Intracranial hemorrhage (ICH) is the most devastating complication in ITP patients. Prophylaxis for ICH is indispensable due to its high mortality. However, the morbidity of ICH is quite low, which makes general prophylaxis unrealistic. A previous study demonstrated risk stratification of ICH in ITP patients before 60 years of age(Platelets, 2020). However, few studies have analyzed the risk factors and outcomes in ICH in elderly ITP patients. Thus, ascertaining the characteristics of ICH in elderly ITP patients is in urgent need to make effective assessments and provide personalized prophylaxis. Here, a retrospective study of a series of ITP patients who developed ICH ≥ 60 years of age was conducted to explore potential risk and prognostic factors, which may contributes to identifying the feasible personalized prophylaxis for ICH in elderly ITP patients.
Patients and methods:
A total of 44 patients incorporated in the study were over 60 years of age with a diagnosis of primary ITP before the onset of ICH. All measures were chronologically performed before the onset of ICH. Univariate and multivariate analyses were conducted using conditional logistic regression model. Each variables with a p-value < 0.10 in the univariate analysis and well-reported factors were included in the multivariate analysis. A stepwise approach was used to exclude variables with a p-value > 0.10.
Results:
Platelet counts at ITP diagnosis were significantly lower among patients who developed ICH afterwards (P=0.004). Platelet counts were dichotomized and coded into binary variables. The cut off value was 25,000/μL according to the ROC curve and Youden index. Estimation by the Kaplan-Meier method indicated that the morbidity of ICH was higher among patients with a baseline platelet count less than 25,000/μL (P=0.001).
Bleeding severity was also included in the analysis. The control group had a significantly higher probability of no bleeding(P=0.008), while the case group was more likely to suffer life-threatening bleeding(P=0.006). The anatomic sites of bleeding manifestations were then examined. There existed significant difference between cases and controls with respect to skin bleeding (P=0.002), oral cavity bleeding (P < 0.001), gastrointestinal bleeding (P=0.022) and hematuria (P < 0.001).
Univariate analysis also revealed that patients with a complication of diabetes mellitus (P=0.007) exhibited a significantly lower incidence of ICH, and fewer patients over 75 years of age developed ICH(P=0.021). Patients who had suffered head trauma before the end point of follow-up had a significantly higher probability of developing ICH (P=0.016). Moreover, patients with a duration of ITP no more than 7 days showed potential relevance (P=0.016).
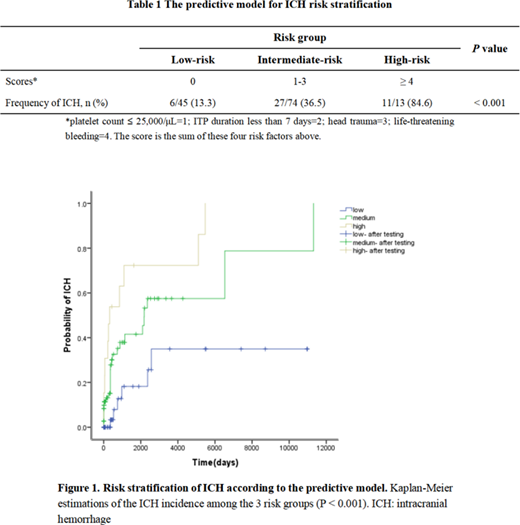
Multivariate analysis was conducted using a conditional logistic regression model. A stepwise approach identified a platelet count ≤ 25,000/μL at ITP diagnosis(OR=3.389, 95% CI 1.290-8.907, P=0.013), head trauma (OR=9.753, 95% CI 1.029-92.414, P=0.047), ITP duration less than 7 days (OR=6.741, 95% CI 1.348-33.712, P=0.020) and life-threatening bleeding(OR=13.077, 95% CI 1.104-154.865, P=0.041) as independent risk factors for ICH in elderly ITP patients. A simple predictive model was established according to the results above. Patients were segregated into a low-risk (Score=0), an intermediate-risk (Score=1-3) and high-risk (Score≥4) groups. Significant differences (P < 0.001) were observed in the frequencies of ICH between the 3 risk groups (Table 1). Kaplan-Meier estimations of ICH incidence were markedly different among the risk groups (Figure 1).
As for prognostic factors, skin bleeding (OR=17.400, 95% CI 1.926-157.190, P=0.011) was identified as an independent poor prognostic factor. No significance was found with respect to age, platelet count or ITP duration.
Conclusion:
Our study revealed that platelet count ≤ 25,000/μL at ITP diagnosis, head trauma, ITP duration < 7 days and life-threatening bleeding are all independent risk factors for ICH in elderly ITP patients. A simple predictive model was established using these factors, and skin bleeding was a poor prognostic factor for ICH in elderly ITP patients.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

