

Background: Chimeric antigen receptor (CAR) T cell therapy is generally limited to inpatient settings; yet, exploration of outpatient infusion and monitoring is ongoing. Information on health care resource utilization (HCRU) and costs associated with CAR T cell therapy administration is limited and may differ by postinfusion monitoring site. Liso-cel is an investigational, CD19-directed, defined composition, 4-1BB CAR T cell product administered at equal target doses of CD8+ and CD4+ CAR+ T cells. An interim analysis from the OUTREACH study (NCT03744676) observed lower HCRU with outpatient vs inpatient administration (Bachier et al. J Clin Oncol 2020;38:8037). The patient journey after CAR T cell therapy administration may differ for patients with outpatient vs inpatient monitoring and may result in varying costs of care. This study estimated the cost of postinfusion monitoring by site of care for patients with R/R LBCL who received third-line or later treatment with liso-cel in the TRANSCEND NHL 001 (TRANSCEND; NCT02631044) and OUTREACH clinical trials.
Methods: This retrospective study analyzed HCRU reported in clinical trial databases from TRANSCEND and OUTREACH. A 2-step microcosting method was used to identify key HCRU and to estimate postinfusion costs: (1) HCRU was analyzed from the index date (day of liso-cel infusion) through the 6-month follow-up; and (2) costs were applied to each HCRU. HCRU included standard inpatient and intensive care unit (ICU) length of stay (LOS), diagnostics (laboratory work and imaging), procedures (dialysis and intubation), and medications (supportive care, prophylactic treatment, and adverse event management). Unit costs were obtained from the health care system (provider) perspective and adjusted to 2020 US dollars. Cost per standard inpatient day ($2,542) was estimated from Healthcare Cost and Utilization Project databases, and cost per ICU day ($7,556) was sourced from Dasta et al (Crit Care Med. 2005;33:1266-77). All medication costs were obtained from REDBOOK (IBM Micromedex) using wholesale acquisition costs. Diagnostic and procedure costs were obtained from the Centers for Medicare & Medicaid Services laboratory fee schedule, physician fee schedule, or outpatient prospective payment system. A payment-to-cost ratio was applied to Medicare payment rates to estimate unit costs. Costs were adjusted to reflect the site of care where the HCRU occurred. A cost ratio was applied to adjust costs from the physician's office/community oncology clinic to the hospital outpatient department (Winfield, Muhlestein, Leavitt Partners; 2017) and from outpatient to inpatient (Meisenberg et al. Bone Marrow Transplant. 1998;21:927-32). Costs were aggregated by HCRU category, specifically medications, diagnostics, procedures, and facility costs. An average total cost by post-liso-cel infusion month was calculated for patients with ongoing status in that month (patients censored due to data cutoff were not included). Analyses were stratified by site of postinfusion monitoring (inpatients vs outpatients).
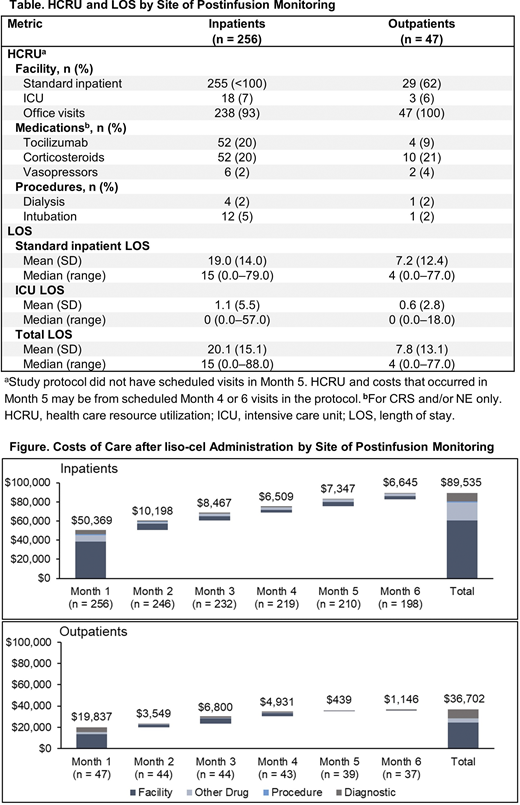
Results: A total of 303 patients with R/R LBCL across the 2 trials received liso-cel and postinfusion monitoring (inpatients, n = 256; outpatients, n = 47). HCRU and LOS, including standard inpatient and ICU days, are shown in the Table. Inpatients had higher rates of inpatient stays (<100% vs 62%) and tocilizumab use (for CRS and/or NE; 20% vs 9%) than outpatients, respectively. Rates of ICU admission, corticosteroid use, vasopressor use, dialysis, and intubation were similar between groups. Median and average LOS in standard inpatient and ICU settings were higher among inpatients. Median (range) total LOS for inpatients and outpatients was 15 (0-88) and 4 (0-77) days, respectively. The estimated mean postinfusion cost of care was $89,535 for inpatients and $36,702 for outpatients. Over 6 months, most costs were incurred in the first month after infusion ($50,369 [56%] for inpatients and $19,837 [54%] for outpatients). Costs were largely driven by facility costs, namely standard inpatient and ICU stays (Figure).
Conclusions: Lower overall HCRU was observed with outpatient liso-cel postinfusion monitoring, primarily due to hospitalizations, which resulted in a mean 6-month cost savings of $52,833 (59%) compared with inpatient monitoring. These results are based on national average costs and may not be generalizable to specific institutions.
Palomba:Regeneron: Research Funding; Juno Therapeutics, a Bristol-Meyers Squibb Company: Honoraria, Research Funding; Genentech: Research Funding; Merck: Honoraria; Novartis: Honoraria; Celgene: Honoraria; Pharmacyclics: Honoraria. Jun:Bristol-Myers Squibb Company: Current Employment, Current equity holder in publicly-traded company. Garcia:Bristol-Myers Squibb Company: Current equity holder in publicly-traded company; Juno Therapeutics, a Bristol-Myers Squibb Company: Current Employment. Lymp:Bristol-Myers Squibb Company: Current equity holder in publicly-traded company; Juno Therapeutics, a Bristol-Myers Squibb Company: Current Employment. McGarvey:Pfizer, Inc.: Ended employment in the past 24 months; BluePath Solutions: Current Employment. Gitlin:BMS: Research Funding. Pelletier:BMS: Current Employment, Current equity holder in publicly-traded company. Nguyen:BluePath Solutions: Current Employment.

