

Background: The features of the IGHV gene repertoire in CLL have been widely discussed in the last 20 years. In approximately 30% of cases of CLL, highly homologous "stereotyped" antigen receptors (SARs) are expressed, representing quasi identical amino acid sequences. Associations with age, disease severity, and cytogenetic aberrations have already been reported for certain SARs. It should be noted that the predictive value of certain SARs could be higher than that of IGHV mutation status. Several SAR subgroups have already been identified as independent prognostic factors in CLL (CLL#1, CLL#2, CLL#8 demonstrate an extremely aggressive course of the disease, CLL#4 - indolent). It was also shown that SAR subgroups may associate with distinct profiles of genetic lesions.
Aim: To study the frequency of cytogenetic aberrations and mutations in the TP53, NOTCH1, and SF3B1 genes in CLL patients with the most common SARs in Russia.
Methods: The study included 62 patients with CLL diagnosed and followed up from 2012 to 2020. Sequencing of the IGHV gene and SAR assignment were done according to the ERIC recommendations. NOTCH1 gene mutations (exon 34) were assessed by fragment analysis or by NGS using primers described by Campregher et al. TP53 gene mutations (exons 2-11) were determined using NGS according to Pavlova et al. SF3B1 gene mutations (exons 14-16) were studied in 26 patients by NGS. 51 patients underwent a FISH study for the presence of 17p13/TP53 deletions; 29 - additionally for 11q23/ATM and 13q14 deletions (Abbott, USA).
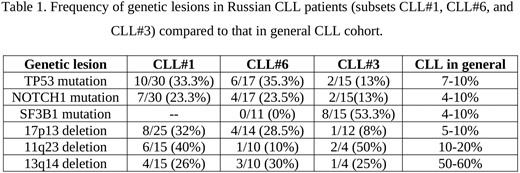
Results: CLL#1, CLL#6, and CLL#3 are the most common SAR subsets in Russian CLL patients. Here we report data for 30 patients with CLL#1, 17 with CLL#6, and 15 with CLL#3. In CLL#1 group, 10 (33.3%) patients had mutations in the TP53 gene. In 7 cases, the mutation burden exceeded 35%, in three patients it was less than 10%. In 7 (23.3%) patients, mutations in the NOTCH1 gene were detected, in 5 - c.7544_7545delCT, in 1 - c.7558_7561delCTTC and in 1 - p.Q2444X. Simultaneous mutations in the NOTCH1 and TP53 genes were found in two patients. Deletion 17p13was found in 8 patients from 25 studied (32%). In 7 patients TP53 mutation and del17p13 were observed simultaneously. Deletion 11q23 was found in 6 out of 15 patients (40%). No cases with the simultaneous occurrence of del11q23 and del17p13 or mutations in the TP53 gene were observed. SF3B1 gene mutations in this group were not investigated. In the CLL#6 group, 6 (35.3%) patients had mutations in the TP53 gene (in two of them two clones with different TP53 mutations were observed). In one case, the mutation was less than 10%. In 4 (23.5%) patients NOTCH1 gene mutations (all c.7544_7545delCT) were detected, in two cases the mutation burden was less than 5%. Simultaneous NOTCH1 and TP53 gene mutations were found in two patients. Deletion 17p13 was found in 4 patients from 14 studied (28.5%). In 3 patients TP53 mutations and del17p13 were observed simultaneously. Deletion 11q23 was found in 1 patient out of 10. No SF3B1 gene mutations were found in this group (in 11 patients tested). In CLL#3 group, only 2 (13%) patients had mutations in the TP53 gene, with one having 2 different clones and the other having 4 (this patient also had del17p13, the only one in this group). Also, only 2 (13%) patients had c.7544_7545delCT deletion in the NOTCH1 gene. SF3B1 gene mutations were found in 8 (53.3%) patients.
Conclusions: Our data show that in CLL#1, CLL#6, and CLL#3 subsets genetic lesions are much more common than in CLL patients in general. This is in part consistent with earlier European studies. However, in our sample, TP53 mutations and del17p13 are much more frequent in CLL#1 and CLL#6 groups. This may be due to a more sensitive approach (NGS) for mutation detection we used. Furthermore, our cohort included patients relapsed after the FCR treatment. The discrepancy in the detection rate of del11q23 in the CLL#1 subset can be explained by the small sample. Also, population differences in the development of the disease cannot be ruled out. Further studies of genetic lesions associated with certain SAR subgroups may improve diagnostics and therapy of CLL and impact the understanding of disease pathogenesis.
No relevant conflicts of interest to declare.

