

Introduction:Hepatic venous occlusive disease (VOD) is a well-described early complication of allogeneic hematopoietic stem cell transplant (HSCT). The disease presents with elevated bilirubin, hepatomegaly, right upper quadrant pain, ascites and weight gain. Multi organ failure (MOF) can also occur, mainly renal and pulmonary failure, in severe cases. The incidence, pathogenesis, risk factors, and treatment of VOD remain poorly defined.
Purpose:We aimed to determine the incidence of, risk factors, treatment patterns and resource utilization associated with VOD in Canada.
Methods:Using the Cell Therapy and Transplant Canada (CTTC) database, which collects data from 15 stem cell transplant programs across Canada, a retrospective observational study was performed. Using patient demographics, disease and transplant characteristics, and the Center for International Blood & Marrow Transplant Research (CIBMTR) Form 2553 which collects information on patients diagnosed with VOD, data was collected. All allogeneic transplants performed on both children and adults between 2013 and 2019 were included in the analysis. Children and adults were analyzed as two separate cohorts.
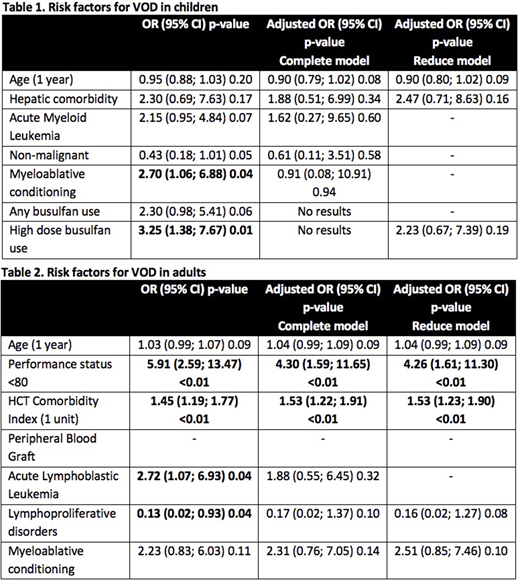
Results:The total incidence of VOD was 64/2507 (2.55%). The incidence of VOD was 27/464 (5.82%) in children and 24/2030 (1.18%) in adults. Risk factors for VOD for children and adults are shown in Tables 1 and 2, respectively. The most common treatments for VOD in children and adults were defibrotide (74.1% and 29.2%, respectively), diuretics (70.4% and 62.5%, respectively) and ursodiol (48.0% and 63.6%, respectively). The mean intensive care unit (ICU) visit duration and hospitalization in children with VOD was 7.0 days and 37.1 days, respectively. The mean ICU visit duration and hospitalization in adults with VOD was 8.2 days and 37.1 days, respectively. There were no differences in overall survival, relapse rates or non-relapse mortality between VOD patients and non-VOD patients in both children and adults.
Discussion:Between 2013 and 2019, the incidence of VOD in allogeneic HSCT in Canada was 2.55%. This is consistent with recent reports from other countries including from the CIBMTR and a report from the United States at 3.3% and 5.4%, respectively. An unexpected finding was the difference in incidence between children and adults. Possible explanations for this include younger age being an actual risk factor for VOD, increased clinical vigilance amongst pediatric clinicians, reporting bias, alternative diagnoses because of more hepatic comorbidities in adults or a more obvious clinical presentation of VOD in children. This requires further investigation. Further to this, a higher proportion of children diagnosed with VOD received defibrotide than did adults diagnosed with VOD. It is unclear why this occurred. The significant risk factors identified in our study are similar to previously published risk factors for VOD. Although, comparative data with non-VOD patients was not available in this data set, VOD patients in both the pediatric and adult populations have longer hospitalizations than historical controls which have an average hospitalization of 23.6 days. No survival or relapse differences were found in our data however VOD cases were not divided into VOD and VOD-MOF. VOD-MOF has been associated with significant mortality of >80%. Weaknesses of our study include its retrospective nature, potential for reporting bias, variable reporting quality from multiple centres and lack of uniform diagnostic criteria for VOD.
Conclusion:The incidence and risk factors for VOD in 15 Canadian HSCT centres are similar to previous reports from other countries. Children made up a higher proportion of VOD patients and a high proportion of children received defibrotide. Further study of the resource utilization associated with VOD is required.
Acknowledgements:Veronique Baribeau and Jean Lachaine of PeriPharm Inc. for data analysis and Jazz Pharmaceuticals for funding, study design, data analysis and editorial contributions.
Paulson:Jazz Pharmaceuticals: Consultancy, Membership on an entity's Board of Directors or advisory committees.

