

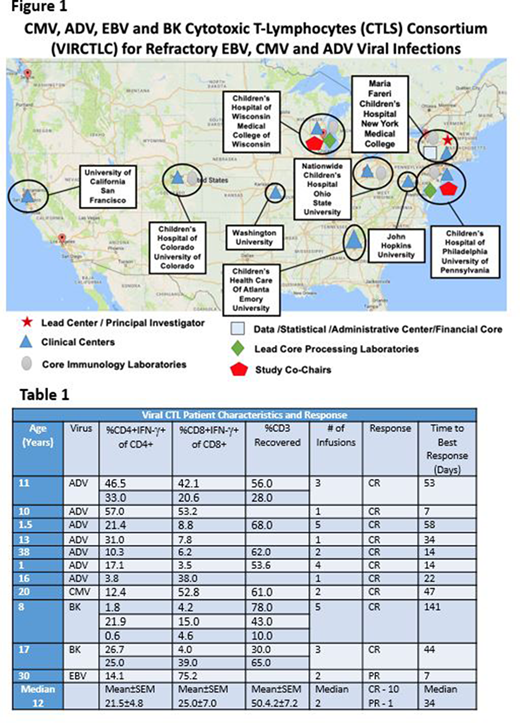
Background: Viral infection remains a major cause of morbidity and mortality after allogeneic hematopoietic stem cell transplantation (allo-HSCT) (Bollard/Heslop Blood 2016). Anti-viral agents for treatment of viral infection in immunocompromised patients are limited in efficacy and are associated with significant toxicities (Gerdemann BBMT 2004; Sili Cytother 2012). The use of virus-specific cytotoxic T-lymphocytes (VST) for immunocompromised patients with viral infections has been associated with therapeutic benefit and improved OS (Bollard/Heslop Blood 2016; Sutrave Cytother 2017). Methods of VST production include ex-vivo expansion and direct selection (Gottlieb Cytother 2017). Ex-vivo expansion requires prolonged manufacturing time, is associated with T-cell exhaustion, and results in a limited donor pool. Direct selection is rapid (12-24 hours), can be done locally, allows for expanded HLA matching, permits a low degree of HLA match to the recipient, and can be adapted for many viruses. A multicenter consortium, the Viral Cytotoxic T-Lymphocyte Consortium (VIRCTLC) was created to investigate the safety and efficacy of VST manufactured by direct selection using the IFN-g Cytokine Capture System process automated on the CliniMACS® Prodigy device (Miltenyi Biotec) for immunocompromised patients with viral infection (Figure 1).
Objective: Determine the safety and efficacy of VST for the treatment of immunocompromised child, adolescent and young adult (CAYA) patients with refractory, systemic viral infection and/or viral infection and intolerance to appropriate anti-viral medical therapy.
Design/Methods: CAYA patients after allo-HSCT, solid organ transplantation (SOT), or with primary immunodeficiency (PID) with refractory adenovirus (ADV), cytomegalovirus (CMV), Epstein Barr virus (EBV) or BK virus (BKV) infections as evidenced by increasing serum RT-PCR DNA (by 1 log) after 7 days or persistent quantitative RT-PCR DNA copies after 14 days of appropriate anti-viral therapy, and/or known resistance to anti-viral agents, and/or intolerance to anti-viral agents were eligible. Related donors with ≥1 HLA A, B, or DR match to recipient and with an adequate T-cell response to virus specific MACS® PepTivators were eligible. Donors were screened with viral specific antigen (PepTivator®) to predict successful VST manufacturing. Peripheral blood mononuclear cells (PBMC) were collected from eligible related donors using non-mobilized apheresis. VST were isolated using the CliniMACS® Prodigy following stimulation of PBMC with specific viral MACS PepTivator® pools, generously provided by Miltenyi Biotec. Production of CD4+ and CD8+ VST was performed as previously described (Feuchtinger Blood 2010). The target cell dose was 0.5x104 CD3+/kg for HLA mismatched haploidentical related donors and 2.5x104 CD3+/kg for matched related donors. Based on response and safety, VST were given every 2 weeks for a maximum of 5 infusions.
Results: Eleven patients have been enrolled to date. Seven patients were treated for ADV, 2 for BKV, 1 for CMV, and 1 for EBV. There were 8 males and 3 females enrolled, aged 1-38 years. There were 10 patients post allo-HSCT and 1 patient post SOT. There were 8 haploidentical, related, original allo-HSCT donors and 3 haploidentical, related, third party donors. There have been no matched related donors enrolled to date. The mean±SEM %CD4+ IFN-g+ of total CD4+, %CD8+ IFN-g+ of total CD8+, and %CD3 cells recovered in the final product were 21.5±4.8, 25.0±7.0, and 50.4.2±7.2, respectively. The median number of VST infusions was 2 (1-5). The mean±SEM CD3+ cell dose was 0.49±0.001x104. Ten patients achieved complete response (PCR negative) and 1 patient achieved partial response (PCR≥1 log decrease). The overall response and complete response rates were 100% and 90.9%, respectively. The median time to maximal response was 34 days (7-141) (Table 1). No patient developed aGVHD, cGVHD, infusion reaction or CRS associated with VST.
Conclusion: Preliminary results of this pilot study demonstrate that VST are safe, well tolerated and efficacious in CAYA with refractory viral infections after allo-HSCT, SOT or with PID. Manufacturing utilizing the CliniMACS® Prodigy device is rapid, reproducible and effective. Accrual is ongoing. This research is supported by FDA RO10063-01A1.
Flower:Lentigen Technology Inc/Miltenyi Biotec: Research Funding. O'Donnell:Kiadis Pharma: Other: Licensing of intellectual property. Lee:Kiadis Pharma Netherlands B.V: Consultancy, Current equity holder in publicly-traded company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties. Johnson:Cell Vault: Research Funding; Miltenyi Biotec: Research Funding. Cairo:Technology Inc/Miltenyi Biotec: Research Funding; Nektar Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding; Miltenyi: Research Funding; Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau.

