

Introduction:
Management of primary CNS lymphoma (PCNSL) in patients age >70 represents a significant challenge. In most clinical series, median OS for PCNSL patients age >70 is <1 year (Mendez et al., Neuro-Oncology 2018). Since late 2011, our group has used low-dose lenalidomide as maintenance therapy in older patients with newly-diagnosed PCNSL who had >partial response (PR) to induction chemotherapy or salvage chemotherapy for relapsed disease. A preliminary report by our group supported the feasibility and efficacy of low-dose lenalidomide maintenance for 13 older patients with PCNSL, in lieu of consolidation with radiation or high-intensity chemotherapy (Vu et. al., BJH 2019).Here, we present the outcomes of 22 consecutive older patients with PCNSL (inclusive of updated outcomes on the original 13 patients) treated with low-dose lenalidomide after achieving >PR following induction chemotherapy. In addition, we provide a first report on the impact of maintenance low-dose lenalidomide on quality of life (QOL), overall functioning, and symptom burden.
Methods:
We performed a retrospective analysis of consecutive patients age >65 years with PCNSL, who achieved >PR to induction methotrexate/rituximab+temozolomide (MTR) chemotherapy and were subsequently treated with low-dose lenalidomide maintenance (5-10 mg/dose) in PR1/CR1. We determined their clinical characteristics, progression-free survival (PFS) and overall survival (OS) by Kaplan-Meier. In addition, we obtained correlative data on QOL and symptom burden on a representative sample of older PCNSL patients who were treated with low-dose IMiDs over the course of > 2 months, via the European Organization of Research and Treatment of Cancer (EORTC) QOL questionnaire (QLQ)-C30. Our study was approved by the University of California San Francisco Institutional Review Board with patient informed consent.
Results:
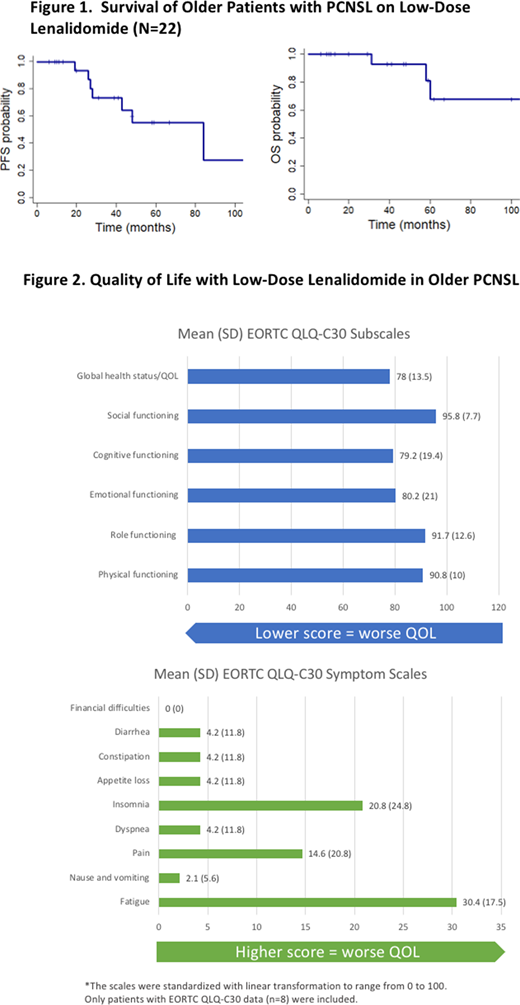
The median age at diagnosis of the 22 consecutive older newly-diagnosed PCNSL patients was 77 (range 64 - 86). Median Karnofsky Performance Status was 70. Twenty patients received induction MTR (2 received M-R) without consolidative dose-intensive chemotherapy, autologous stem cell transplant, or whole brain irradiation. The median methotrexate dose was 2.5 gm/m2 (range 0.5 - 8). With median follow-up of 47 months, median time on low-dose lenalidomide maintenance was 14 months. Median PFS was 84 months, and median OS has not been reached. (Figure 1). At progression, patients received methotrexate followed by lenalidomide or pomalidomide. Thus far, there have been 3 deaths: one due to PCNSL, one by myocardial infarction, 4 years after discontinuation of lenalidomide, and one without definitive cause.
To assess the tolerability of low-dose lenalidomide (and/or pomalidomide) in this population, we determined patient-reported outcomes with respect to quality of life, as measured by the EORTC QLQ-C30. We summarize our findings in Figure 2 on 8 consecutive PCNSL patients age >70 that received maintenance IMiD therapy for at least 2 months. Seven of the 8 patients were treated with maintenance low-dose lenalidomide for a median of 11 months, and one patient was on maintenance pomalidomide (1-2 mg/day) for a total of 76 months. Overall low-dose IMiDs were well-tolerated: mild-to-moderate fatigue and insomnia were the two most commonly reported symptoms.
Conclusions:
Our experience suggests that low-dose lenalidomide as maintenance therapy after induction chemotherapy in older patients with PCNSL may result in improved PFS and OS. Importantly, our data suggest that QOL and overall functioning as measured by the EORTC QLQ-C30 was comparable, if not better, than QOL as assessed for patients receiving high dose methotrexate-based therapy, autologous stem cell transplant, whole brain radiation therapy, and/or blood brain barrier disruption (Doolittle et. al., Neurology 2013). In conclusion, based on this preliminary assessment, maintenance low-dose lenalidomide (and pomalidomide) appear to be well-tolerated in older PCNSL, with patients reporting good quality of life, low symptom burden, and overall good level of functioning. Survival outcomes remain encouraging. A phase I trial in newly-diagnosed, non-transplant eligible PCNSL that evaluates combination nivolumab with lenalidomide, both as a component of induction therapy and as low-dose lenalidomide maintenance, is in development via Alliance (A051901).
Rubenstein:Kymera: Research Funding.
Low-Dose Lenalidomide as Maintenance in Older Patients with Primary CNS Lymphoma

