


Background: Hypercoagulability may contribute to COVID-19 pathogenicity. Evidence comparing clinical outcomes among patients with COVID-19 receiving therapeutic compared to prophylactic dose anticoagulation is limited. We evaluated whether therapeutic anticoagulation (tAC) is associated with improved survival compared to prophylactic (pAC) and no anticoagulation (AC) in hospitalized COVID-19 patients.
Methods: This was a retrospective, multi-center cohort study of consecutive COVID-19 patients admitted between March 13th, 2020 and May 5th, 2020 to eight hospitals within a large academic system in Southeast Michigan, USA. Participants were assigned to three groups based on whether they received no AC, pAC throughout most of their hospitalization, or at least 3 days of tAC. Major bleeding was defined as transfusion of five or more units of packed red blood cells within 48 hours regardless of hemoglobin level, hemoglobin < 7g/dL and any red blood cell transfusion or a diagnosis code for major bleeding during the hospitalization or radiological evidence of intracranial hemorrhage
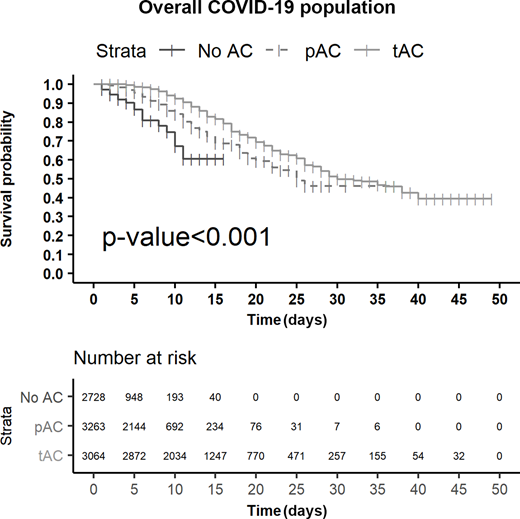
Results: A total of 3480 patients were included (mean age, 64.5 years [17.0]; 51.5% female; 52.1% black and 40.6% white). 18.5% (n=642) were treated in the intensive care unit (ICU). 60.9% received pAC (n=2121), 28.7% received at least 3 days of tAC (n=998), and 10.4% (n=361) did not receive AC. Propensity score (PS) weighted Kaplan-Meier plot demonstrated a statistical difference in the 25-day survival probability in the tAC group compared to the pAC group (57.5% vs 50.7%, Figure). In a PS weighted multivariate proportional hazards model adjusting for age, body mass index and ICU status, AC was associated with a reduced risk of death at both prophylactic (hazard ratio [HR] 0.35 [95% confidence interval {CI} 0.22-0.54]) and therapeutic doses (HR 0.14 [95% CI 0.05-0.23]) compared to no AC. Major bleeding occurred more frequently among tAC patients (81 [8.1%]) compared to those who received no AC (20 [5.5%]) or pAC (46 [2.2%]).
Conclusions: Higher doses of AC are associated with lower mortality in hospitalized COVID-19 patients. The lowest hazard ratio was observed in ICU patients, but risk was also significantly lower in non-ICU hospitalized patients. Bleeding occurred more frequently with higher doses of anticoagulation. Ongoing randomized trials are warranted to prospectively evaluate efficacy and risk of tAC in patients with COVID-19.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

