

Introduction:
Despite more than 80% long-term survival in acute lymphoblastic leukemia (ALL), morbidity due to drug-related toxicities remains high. Treatment interruptions and omissions from these toxicities may affect survivorship outcomes and morbidities in pediatric cancer. Although multiple factors contribute to a patient's risk of toxicity pharmacogenetic factors have been shown to play critical roles. Genetic variation within genes involved in pharmacokinetic and pharmacodynamic pathways of chemotherapies can influence gene expression and/or activity resulting in inter-patient variation in drug levels and thus toxicity risk or therapeutic efficacy. Identification of SNPs of clinical relevance that are predictive of toxicity can allow clinicians to optimize therapy to manage toxicity phenotypes.
Objective:
The objective of this cross-sectional study was to explore pharmacogenomic biomarkers associated with clinically relevant toxicity phenotypes in children receiving ALL therapy.
Methods:
The protocol was approved by the University of Florida (UF) Institutional Review Board (IRB201802623). All participants provided informed consent. Patients ≤ 26 years of age with a diagnosis of de novo or secondary ALL and who had received induction and consolidation chemotherapy after May 2012 at UF were eligible for participation. Chart review was performed and CTCAE-graded toxicity data was abstracted for gastrointestinal (GI), neurological, and endocrine toxicities along with prolonged hospitalization (> 4 days) due to febrile neutropenia. Genomic DNA was obtained from peripheral blood. SNPs in candidate pharmacological genes in cytarabine, vincristine, methotrexate, daunorubicin/doxorubicin, mercaptopurine/thioguanine pathways were selected through literature search and PharmGKB database. Genotyping was performed using Sequenom-based based chemistry. SNPs with low call rate and minor allele frequency of <0.10 were filtered and 105 SNPs were tested for association with each toxicity endpoint using logistic regression models with additive, dominant, and recessive modes of inheritance. Odds ratio (OR) and 95% confidence interval were calculated for each test. SNPs with association P-value < 0.05 were considered significant.
Results:
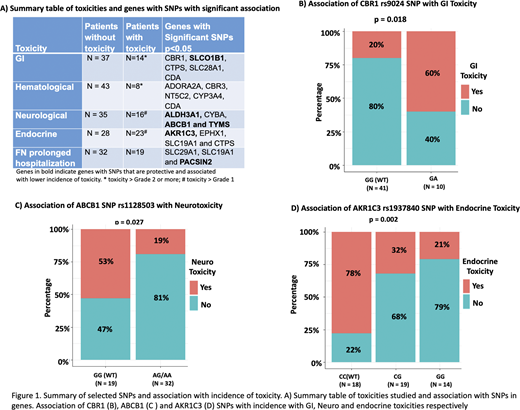
Prevalence of toxicity and top genes with significant SNPs are summarized in Figure 1. SNP in a carbonyl reductase (CBR1) involved in anthracycline metabolism was associated with higher risk of GI toxicity (OR 2.49, p=0.016). Multiple SNPs in cytarabine pathway genes were associated with increased risk of GI toxicities (rs12067645 in CTPS1, rs11853372 in SLC28A1 and rs10916819 in CDA) whereas SNP in an influx transporter SLCO1B1, implicated in methotrexate uptake was associated with lower risk of GI toxicity (rs2291075, OR 0.224, p =0.017). Six SNPs were associated with higher incidence of hematological toxicity with most interesting SNP being rs12067645 in CTPS1, a gene involved in cytarabine metabolism (OR 5.89, p=0.026). rs1128503 in drug efflux transporter ABCB1, rs2228110 in ALDH3A1, and rs2853539 in TYMS were all associated with lower incidence of neurologic toxicities. rs4673 in CYBA (OR 3.76, p=0.015) associated with higher neurological toxicity. Of the 5 SNPs associated with endocrinopathies, 4 were associated with increased and one with reduced incidence of toxicity. Interestingly, 2 SNPs in cytarabine uptake transporter SLC29A1, rs507964 (OR 2.89, p=0.02) and rs324148 (OR 1.89, p=0.042) and one missense SNP rs1051266 in SLC19A implicated in methotrexate influx was predictive of prolonged hospitalizations from febrile neutropenia. Figure 1 highlights some of these results.
Conclusion:
In conclusion, we identified common SNPs in genes associated with pharmacology of most commonly used anti-leukemic agents that were predictive of interpatient variability in incidence of drug toxicity phenotypes in a pilot cohort of 51 patients with ALL. Though limited by sample size, our studies demonstrate exciting results with ongoing enrollment and analysis showing promise in developing a SNP based model for prediction of toxicity in pediatric patients. Our goal is to integrate SNPs into a toxicity score for each patient which, once validated in collaborative multi-site cohorts, will hold value when transitioned to the clinic for personalizing treatment regimens to achieve therapeutic benefit and minimize morbidities.
No relevant conflicts of interest to declare.

