

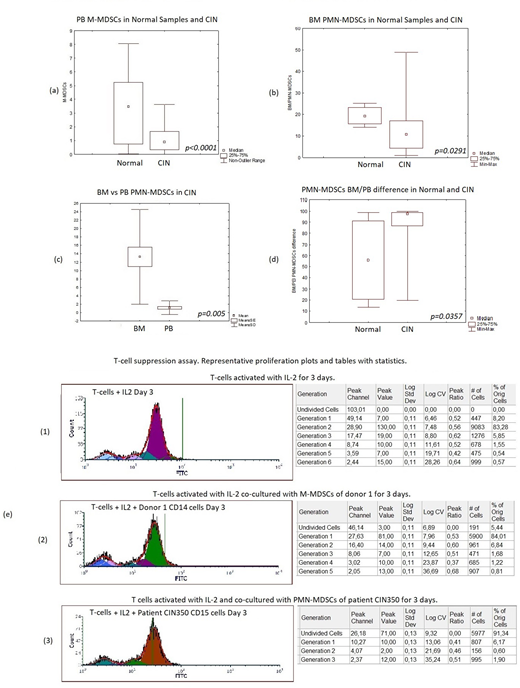
Myeloid-derived suppressor cells (MDSCs) are myeloid cells with immunoregulatory properties characterized mainly by suppression of T-cell responses (Bizymi et al, HemaSphere 2019). They are divided in HLA-DRlow/-/CD11b+/CD33+/CD15+ polymorphonuclear (PMN-MDSCs) and HLA-DRlow/-/CD11b+/CD33+/CD14+ monocytic (M-MDSCs) subsets and they are implicated in inflammatory and malignant diseases. Chronic idiopathic neutropenia (CIN), is a (usually benign) neutrophil disorder characterized by persistent and unexplained neutropenia following a detailed clinical/laboratory investigation including anti-neutrophil antibody testing, bone marrow (BM) biopsy and karyotype (Dale & Bolyard, Curr Opin Hematol 2017). Previous studies have shown that neutropenia in CIN is associated with increased apoptosis of BM granulocytic progenitor cells due to an inflammatory BM microenvironment consisting of oligoclonal T-lymphocytes, proinflammatory monocytes and proapoptotic cytokines. The aim of the present study is to explore the possible involvement of the MDSCs in the pathophysiology of CIN by investigating their number in peripheral blood (PB) and BM in association with their functional characteristics. We have studied 100 CIN patients and 49 age- and sex-matched healthy controls. The patients fulfilled the previously described diagnostic criteria for CIN (Papadaki et al, Blood 2003) and had mean neutrophil counts 1095.67 ± 479.52 (median 1215, range 100-1700). MDSC subsets were quantitated by flow cytometry in the PB mononuclear cell (PBMC) fraction using the combination of CD33PC7/CD15PC5/HLA-DRECD/CD14PE/CD11bFITC monoclonal antibodies and the Kaluza analysis software. MDSC subsets were also studied in the BMMC fraction of 24 CIN patients and 8 healthy controls from the study population. The T-cell suppression function of patient MDSCs was evaluated in coculture experiments of immunomagnetically sorted, CFSE stained, normal CD3+ cells with immunomagnetically sorted M-MDSCs and PMN-MDSCs from 4 patients and 4 healthy donors using recombinant human IL-2 as activating factor. CFSE staining was detected in the CD3+ cells on day 0 and day 3 of coculture and analysis was performed with the Fcs Express 7 software. Statistical analysis was performed with the Statistica software. We found that the proportion of PB M-MDSCs was statistically significant lower in CIN patients (1.45% ± 1.82%) compared to controls (3.68% ± 3.12%, Mann-Whitney test, p < 0.0001) (Figure a) whereas the proportion of PB PMN-MDSCs, although lower in patients, did not differ significantly from the controls. The proportion of BM M-MDSCs did not differ significantly between CIN patients and controls whereas the proportion of BM PMN-MDSCs was statistically significant lower in patients (13.27% ± 11.27%) compared to controls (19.49% ± 4.46%; Mann-Whitney test, p = 0.0291) (Figure b). Paired analysis showed that the proportion of PMN-MDSCs were higher in the BMMC compared to PBMC fraction in both CIN patients (13.27% ± 11.27% vs 1.14% ± 1.64%, respectively; Wilcoxon test, p = 0.005) (Figure c) and healthy controls (19.49% ± 4.46% vs 9.92% ± 9.08%, respectively; Wilcoxon test, p = 0.0118). Interestingly, the proportion of increase of PMN-MDSCs (in BMMC vs PBMC fraction) was significantly higher in patients (86.71% ± 21.26%) compared to controls (55.95% ± 38.59%; Mann-Whitney test, p = 0.0357) (Figure d). The above data indicate low production of PMN-MDSCs in CIN patients compared to controls but a trend for accumulation of these cells in patients' BM. No statistically significant difference was documented in paired analysis of M-MDSCs between BMMC and PBMC fractions in either CIN patients or healthy controls. Patient PMN-MDSCs and M-MDSCs displayed normal capacity to suppress T-cell proliferation as was indicated by the T-cell generations in coculture experiments of normal CD3+ cells in the presence or absence of patient MDSCs (Figure e). In conclusion, CIN patients display low proportion of MDSCs in the PB and lower proportion of PMN-MDSC in the BM compared to normal individuals. Patient MDSCs display normal capacity to suppress T-cell activation. The low proportions of MDSCs may sustain the inflammatory process associated with CIN whereas the accumulation of PMN-MDSCs in the BM represents probably a compensatory mechanism to suppress the inflammatory processes within patients' BM microenvironment.
Papadaki:Genesis pharma SA: Membership on an entity's Board of Directors or advisory committees, Research Funding.

