

Introduction: The increasing prevalence of obesity has not spared the hemophilia population with rates similar to those in the general population. Obesity alters the pharmacokinetic properties of many drugs making it difficult to determine the appropriate dose when administering medications based on total body weight (TBW). Alternative descriptors of body weight, such as lean body mass (LBM) and ideal body weight (IBW) are sometimes used in these situations. Under-or overdosing of clotting factor concentrates in hemophilia may have catastrophic consequences. It has been demonstrated that when recombinant factor VIII (rFVIII) is dosed according to TBW in overweight and obese hemophiliacs, FVIII recovery values are greater than the expected 2.0 IU/dl per IU/kg. These findings suggest the need for alternative methods of rFVIII dosing in individuals whose morphometric characteristics differ from the ideal.
Methods: We performed a single-center, randomized, controlled, open-label, crossover trial to determine if rFVIII dosing based on LBM and IBW achieves a targeted FVIII recovery with better precision than based on TBW in overweight and obese (body mass index ≥25 mg/m2), adult males (age ≥18) with hemophilia A (FVIII activity ≤0.40 IU/dl). Participants were randomized to 1 of 6 possible dosing sequence scenarios based on 3 different weight-based dosing regimens (TBW, LBM, and IBW). Recombinant FVIII dosing was calculated based on weight and a targeted FVIIII recovery of 2.0 IU/dl per IU/kg. Each subject administered his own rFVIII on three separate weeks following a washout period of at least 72 hrs. FVIII recovery was determined using the one-stage clotting assay obtained before and 30 min after infusion. Outcomes consisted of FVIII recovery and the proportion of participantsachieving a targeted FVIII recovery of 2.0 +/- 0.2 IU/dl per IU/kg 30 min after infusion. An intention-to-treat analysis was performed using mixed effects linear and logistic regression with random subject effect adjusted for week.
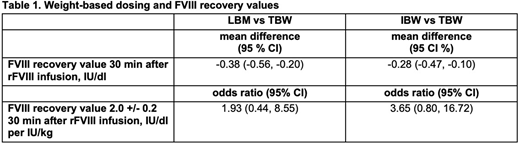
Results: Between September 2015 and March 2019, 30 eligible patients were randomized to 1 of 6 rFVIII weight-based dosing scenarios consisting of TBW, LBM, and IBW. Nineteen participants completed the study. The mean age of participants was 34.6 +/- 11.3 years. The average body mass index (BMI) of participants was 29.2 +/- 3.5 kg/m2. Twenty-six participants had severe hemophilia A and 2 participants each had moderate and mild hemophilia A. Of those receiving at least 1 dose of rFVIII, Eloctate, 66.7%, Advate, 14.3%, and Novoeight, 9.5%, were the most commonly administered products. The mean FVIII recovery for TBW, LBM, and IBW-based dosing was 2.45 (95% CI: 2.27, 2.64), 2.08 (95% CI: 1.89, 2.26), and 2.17 (95% CI: 1.99, 2.35) IU/dl per IU/kg, respectively. The mean FVIII recovery was higher in TBW vs LBW and IBW-based dosing (Table 1).The proportion of participants with a targeted FVIII recovery of 2.0 +/- 0.2 IU/dl per IU/kg was 0.25 (95% CI; 0.09, 0.52), 0.39 (95% CI: 0.18, 0.64), and 0.54 (95% CI: 0.30, 0.77) for TBW, LBM, and IBW-based dosing, respectively. There was no difference in the proportion of participants with a targeted FVIII recovery of 2.0 +/- 0.2 IU/dl per IU/kg in TBW vs LBM and IBW-based dosing (Table 1).
Discussion: In this study, rFVIII dosed according to TBW resulted in a higher FVIII recovery value than LBM and IBW-based dosing in overweight and obese, adult males with hemophilia A. There was no significant difference in the proportion of participants with a targeted FVIII recovery of 2.0 +/- 0.2 IU/dl per IU/kg in TBW vs LBM and IBW-based dosing; however, effect estimates favor alternative dosing strategies with LBM and IBW-based dosing 1.93 and 3.65 times, respectively, having greater odds of achieving targeted FVIII recovery. This may be due to limited statistical power as only 79.2% of the necessary number of participants completed the study. In addition, the rFVIII dose was erroneously calculated in 7 participants resulting in the administration of a smaller than intended amount. This primarily affected IBW and LBM-based dosing, which may have served to reduce the effect size above. In conclusion, based on these findings, overweight and obese patients with hemophilia A should undergo individualized pharmacokinetic studies using alternative descriptors of body weight to determine the most accurate, and cost-effective, method of achieving targeted FVIII recovery values.
Seaman:Takeda: Consultancy; Genentech: Consultancy; Spark Therapeutics: Consultancy; Bayer: Consultancy. Ragni:Alnylam Pharmaceuticals Inc., Baxalta/Takeda, BioMarin, Bioverativ, and Spark Therapeutics: Membership on an entity's Board of Directors or advisory committees; Sangamo: Consultancy, Research Funding; Takeda: Research Funding; Alnylam/Sanofi, ATHN, BioMarin, Bioverativ, Sangamo, Spark: Research Funding; Bioverativ: Consultancy, Research Funding; Spark: Consultancy, Research Funding; BioMarin: Consultancy, Research Funding; Alnylam/Sanofi, BioMarin, Bioverativ, Spark: Consultancy; American Thrombosis Hemostasis Network: Other: Committee work; Baxalta/Takeda, CSL Behring, Genentech, a member of the Roche Group, OPKO Biologics, and Vascular Medicine Institute: Research Funding.

