

Introduction
Priapism is a persistent erection of the penis that is not associated with sexual stimulation or desire lasting more than 4 hours. Priapism can be classified as ischemic, non-ischemic, or stuttering. Stuttering priapism is defined as recurrent priapism lasting less than 4 hours. Commonly, no cause is identified, secondary causes include medications specially intracorporal injections or medical conditions such as hematological diseases particularly sickle cell disease, but it is uncommon to be seen with essential thrombocythemia (ET). It adversely affects the quality of life, sexual function, and physical wellness of the affected patients besides the risk of penile fibrosis and permanent erectile dysfunction. The underlying pathophysiology is not clearly understood but the mechanism involves disturbed nitrous oxide, phosphodiesterase enzyme activity, and disturbed auto-regulation of the penile circulation.
Method
Literature searched in google scholar, PubMed, and Scopus search engines with keywords priapism, essential thrombocythemia, essential thrombocytosis results found from 1960 to 2020.
Results
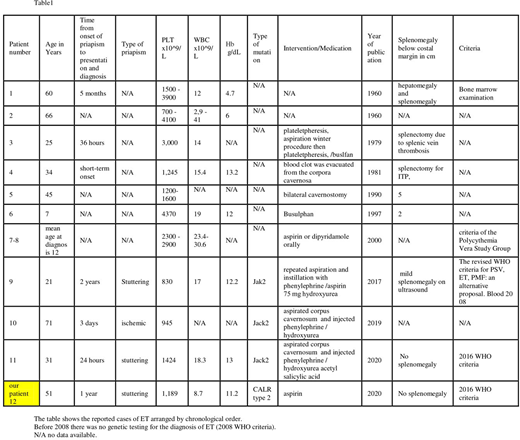
Using the keywords above we found 11 cases of ET devolved or presented with priapism. With the case in our center (not published) the total number of cases will be 12. The cases arranged by chronological order. Almost all age groups are involved from 7 years to 71 years. The table shows hematological parameters, type of mutation, and the management of priapism.
Discussion
In ET the mechanism of priapism is probably related to high platelet count and platelets sludging in the corpora cavernosa, similar to RBC sludging in sickle cell disease and WBC sludging in leukemia. Subsequent stasis and disturbed NO and cGMP signaling. This might be precipitated by increased viscosity or release of free hemoglobin secondary to hemolysis similar to sickle cell anemia as many patients had low hemoglobin levels (table-1). Looking at the table with the available data most hemoglobin levels are in the lower normal limits, but no patient had high hemoglobin levels, opposite to what can be expected that polycythemia might enhance the viscosity of the blood and enhance thrombosis. Observing other MPN who developed priapism, in one study 430 patients with CML 8 patients developed priapism at diagnosis, they had lower hemoglobin levels compared to CML patients who didn't develop priapism. The mean hemoglobin level in patients with priapism was 8.4 ± 2.3 g/dL, compared to 10.8 ± 2.5 g/dL in CML patients control who didn't develop priapism. To the best of our knowledge, there are no reports of cases of adults with polycythemia Vera who devolved priapism which might indicate that anemia has a synergistic effect with leukocytosis in the pathogenesis of priapism in CML patients. But, it is difficult to generalize this observation to ET. However, anemia can enhance thrombosis and the risk of thromboembolism by different mechanisms not related to reactive thrombocytosis. Some patients presented after years from the onset of priapism. This may indicate the complaint of priapism is underreported especially for patients with stuttering priapism who develop erection for a shorter duration of time and subsides spontaneously. While patients with ischemic priapism have prolonged, painful erection usually seeks medical attention from the first time. This can be the reason that CML reports of priapism are relatively more common 1.9 % compared to ET because CML type is predominantly ischemic. At the same time, ET can be ischemic or stuttering.
Most of these cases are reported before 2008 WHO criteria for ET, which explains why no genetic studies done for the cases. This case is the first reported case of CLAR mutation associated with priapism. In the table 6/12 had splenomegaly or splenectomy a ratio close to general ET patients.
Conclusion
Priapism is a rare presentation and complication of ET. It can present as ischemic or stuttering types. ET with stuttering priapism might be underreported. The main risk factors aren't clear due to old and few reported cases. Splenomegaly, age, and type of mutation appear to have little impact. But the characteristic features are the high platelet count and lower hemoglobin level.
No relevant conflicts of interest to declare.

