

Introduction
Breast Implant Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) is a rare subtype of ALCL that arises as a seroma or a mass in the space surrounding textured breast implants. In July 2019 the FDA had reported 573 cases worldwide and 33 deaths connected to the lymphoma. However, collections of cases usually come from large groups of institutions or countries, with different approaches regarding surgery and treatment. Here we describe a cohort of 18 cases undergoing implant removal and capsulectomy and followed at Memorial Sloan Kettering Cancer Center (MSKCC)
Methods
We retrospectively analyzed all the cases of women with breast implants undergoing implant removal and capsulectomy for BIA-ALCL at MSKCC from January 2011 to June 2020. Results are expressed in absolute numbers and percentages, survival is calculated with the Kaplan Maier method.
Results
Of 27 total BIA-ALCL cases seen at MSKCC, 18 women had their primary surgery for implant removal and capsulectomy by our surgery division, analyzed in our central pathology and treated and/or expectantly monitored in our T cell lymphoma clinic. Sixteen patients (89%) had implants as reconstruction after breast cancer (of which 12/16, 75% had received adjuvant/neoadjuvant chemotherapy (CT), 3, 19% radiotherapy (RT). Two subjects (11%) had implants for cosmetic reasons). Four patients (25%) had undergone implants exchange after initial reconstruction. BRCA mutational status was known in 9 patients (56%), with 3/9 women (33%) having BRCA mutations (2 BRCA2, 1 BRCA1) and one additional woman initially thought to have a mutation of BRCA2, subsequently re-classified as polymorphism.
After a median exposure of 11 years (STDEV 6 y), 10 years from last implant change, median age at BIA-ALCL diagnosis was 57 years (STDEV 10 y). Implant characteristics were as follows: 18/18 (100%) silicone surface, 17/18 (94%) had a biocell textured surface, 1/18 (6%) unknown surface, 9/18 (50%) silicone filled, and 9/18 (50%) saline filled.
BIA-ALCL presented as effusion in 14/18 (78%) of cases, mass in 3/18 (17%) of cases, and PET+ intramammary lymphadenopathy in 1/18 (6%). Pre-surgery, cases were assessed with PET/CT in 15/18 (83%), US in 15/18 (83%) and MR in 7/18 (39%).
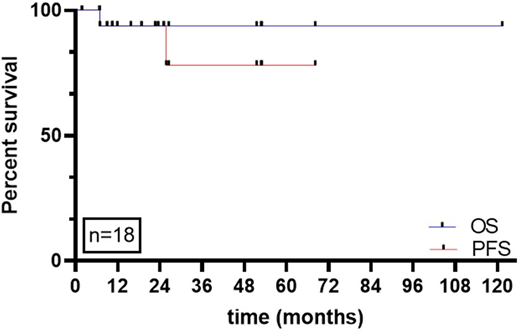
Initial treatment was implant removal and capsulectomy for all women, with removal of all the implants in place. One early case received implant removal and replacement with a smooth textured implant with partial capsulectomy prior to confirmed diagnosis. Three of 18 (16%) who presented with higher stage disease received additional treatment: one received chemotherapy (Brentuximab Vedotin - cyclophosphamide - doxorubicin - prednisone, BV-CHP) followed by RT consolidation, and 2 received RT consolidation only. Patients were followed for a median of 26 months (STDEV 2.22 months) after diagnosis, with clinical exam every 3-6 months (100%), PET/CT in 16/18 (89%), and MR in 4/18 (22%). No patient died of lymphoma progression or recurrence. One patient died from progression of breast cancer. One woman (described above) recurred 2 years after receiving incomplete capsulectomy and smooth surface implant re-placement. She underwent repeat implant removal and bilateral capsulectomy and remains disease free at 6.5 years from the second surgery. Another patient was likely diagnosed at recurrence: she underwent unilateral implant removal and partial unilateral capsulectomy for recurrent delayed seroma (at the time of this implant removal BIA-ALCL could not be confirmed). 1.5 years later she developed a recurrent seroma on the contralateral side where a textured device remained. BIA-ALCL diagnosis was confirmed at this time. Overall survival (Figure 1), was 94% at 2 years and progression-free survival was 89% at 2 years.
Conclusions
Our data on this cohort of patietns with BIA-ALCL surgically treated and followed at a single institution, confirm the importance of adequate surgery (bilateral implant removal and complete capsulectomy) in patients presenting with seroma-confined disease. This dataset reinforces the high rates of progression free and overall survivalwhen diagnosis is identified and treatment performed in those with limited stage disease. Studies are ongoing to determine the role of somatic mutations like BRCA1-2.
Figure: overall and progression-free survival of BIA-ALCL women operated and followed at MSKCC
Cordeiro:Inamed: Consultancy, Research Funding; Acelity: Consultancy; Allergan: Consultancy, Research Funding. Moskowitz:Bristol-Myers Squibb: Research Funding; Merck: Research Funding; Merck: Consultancy; Miragen Therapeutics: Consultancy; Seattle Genetics: Consultancy; Seattle Genetics: Research Funding; Incyte: Research Funding; Imbrium Therapeutics, L.P.: Consultancy. Dogan:Takeda: Consultancy; AbbVie: Consultancy; National Cancer Institute: Research Funding; Seattle Genetics: Consultancy; EUSA Pharma: Consultancy; Corvus Pharmaceuticals: Consultancy; Roche: Consultancy, Research Funding; Physicians Education Resource: Consultancy. Horwitz:Vividion Therapeutics: Consultancy; Affirmed: Consultancy; Daiichi Sankyo: Research Funding; GlaxoSmithKline: Consultancy; Janssen: Consultancy; Kura Oncology: Consultancy; ASTEX: Consultancy; C4 Therapeutics: Consultancy; Beigene: Consultancy; Portola: Consultancy, Research Funding; Mundipharma: Consultancy; Innate Pharma: Consultancy; Corvus: Consultancy; Trillium: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; Millenium/Takeda: Consultancy, Research Funding; Kyowa Hakka Kirin: Consultancy, Research Funding; Infinity/Verastem: Research Funding; Forty Seven: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Aileron: Consultancy, Research Funding; ADCT Therapeutics: Consultancy, Research Funding; Verastem: Consultancy, Research Funding; Myeloid Therapeutics: Consultancy; Miragen: Consultancy.

