

Background: The clinical features and prognosis of adult Langerhans cell histiocytosis (LCH) remained poorly defined. Although recurrent somatic activating mutations of BRAFV600E and additional genetic drivers of MAPK pathway had been discovered in LCH, most genomic analyses were from children and the spectrum of genetic alterations and the impact of these genetic mutations on clinical presentation in adult LCH remains elusive. To address these questions, we retrospectively studied the clinical features, organ involvement, treatment approaches, genomic analyses and outcomes of adult LCH patients in our center.
Methods: Patients diagnosed with LCH between January 2001 and June 2020 at Peking Union Medical College Hospital were included in this retrospective study. BRAF or MAP2K1 mutation was detected by a custom-designed NGS panel. Patients were classified according to the number of systems involved: SS-s, one lesion in a single system; SS-m, multiple lesions within one single system; and MS, multiple systems involved. The overall survival (OS) was defined as the duration from the diagnosis of LCH to the date of death. The event free survival (EFS) was defined as the duration from the initiation of treatment for LCH to reactivation after treatment and death from any cause.
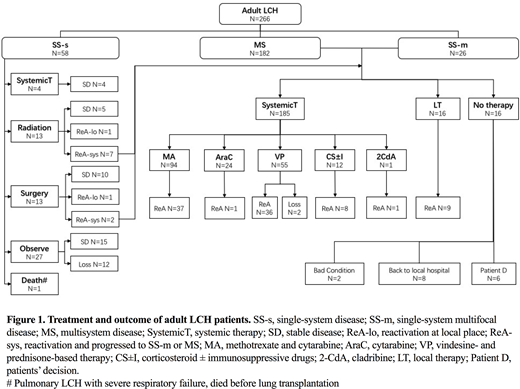
Results: Overall 266 patients were enrolled, 177 patients were male (66.5%). The median age at diagnosis was 32 years (range, 18-79 years). At the time of diagnosis, 58 patients had SS-s LCH (21.8%), 26 patients had SS-m LCH with bone involvement (9.8%) and 182 patients had MS LCH (68.4%). The most common organ involved in MS patients was bone (69.8%), followed by the pituitary (61.5%), lung (61.0%), lymph nodes (35.2%), skin (26.4%), liver (23.1%), thyroid (13.7%), spleen (8.2%), CNS (3.8%) and gastrointestinal tract (1.1%). No patients had hematopoietic system involvement. For 67 patients, BRAF and MAP2K1 mutation status were successfully determined with NGS. BRAFV600E was detected in 26 patients (38.8%), BRAFV600D was detected in 1 patient (1.5%), BRAFT599I in 1 patient (1.5%) and BRAFdeletion mutation in 17 patients (25.4%), including 15 BRAF N486_P490 and 2 BRAF N486_P491delinsS. MAP2K1 mutation was detected in 13 patients (19.4%). BRAF status was related to disease features and extent of disease. BRAF deletion was found in 38.5% of patients with MS LCH, 7.1% of patients with SS LCH (P= 0.004). BRAF deletion was apparent in 69.2% of patients with liver involvement (P <0.001). While bone involvement was associated with BRAFV600E mutation (46.2% vs 13.2%, P = 0.033). The initial treatment of the whole cohort is illustrated in the flow diagram of Figure 1. The estimated 4-year OS and EFS of patients with SS-s LCH were 97.2% and 57.0%, respectively. Totally 201 MS or SS-m patients received first-line treatment at our hospital. After a median 43-month follow-up (range 1-214 months), 92 patients had reactivation. The median EFS was 38.5 months (95% CI, 20.9-56.1 months). To evaluate the prognostic factors of EFS using multivariate Cox regression model, the involvement of liver (HR 0.545, 95% CI 0.335-0.885) or spleen (HR 0.416, 95% CI 0.205-0.844) at baseline were predictive of poor EFS, while receiving cytarabine-based therapy as a first-line treatment (HR 2.195, 95% CI 1.441-3.344) and age older than 30 years at diagnosis (HR 1.660, 95% CI 1.087-2.533) predicted favorable EFS. BRAF or MAP2K1 mutation status did not significantly affect EFS. Seventeen patients died during follow-up. The estimated 4-year OS was 94.4% of patients with MS or SS-m.
Conclusion: We first found more than 25% of adult LCH patients carried BRAFdeletion (BRAF N486_P490 or BRAF N486_P491delinsS), which was related with MS and liver involvement. Also, we demonstrated that liver and spleen involvement indicates a worse prognosis in adult LCH, age older than 30 years at diagnosis predicted favorable EFS and a cytarabine-based regimen should be considered as a first-line treatment for adult MS or SS-m LCH patients.
No relevant conflicts of interest to declare.

