


Introduction: New targets and treatment modalities are needed for multiple myeloma (MM). Fc receptor-homolog 5 (FcRH5) is a type I membrane protein that is expressed on B cells and plasma cells, and is found on myeloma cells with near 100% prevalence. BFCR4350A, a humanized immunoglobulin G-based T-cell-engaging bispecific antibody (bsAb), targets the most membrane-proximal domain of FcRH5 on myeloma cells and CD3 on T cells. Dual binding facilitates efficient immunological synapse formation, resulting in T-cell activation and potent killing of myeloma cells (Li et al. Cancer Cell 2017). GO39775 (NCT03275103) is an ongoing, multicenter Phase I trial evaluating the safety, activity, pharmacodynamics, and pharmacokinetics of BFCR4350A monotherapy in pts with relapsed/refractory (R/R) MM. We present dose-escalation data from the single step-up dosing cohort (Arm A).
Methods: All pts have R/R MM for which no established therapy is available, appropriate, or tolerated. Prior exposure to CAR-T cells, T-cell engaging bsAbs, and antibody-drug conjugates (ADCs), including those targeting BCMA, is allowed. In dose-escalation, pts receive BFCR4350A by IV infusion in 21-day cycles (Q3W). In Arm A, a single step-up dose is used in Cycle (C) 1 to mitigate the risk for cytokine release syndrome (CRS), with the step dose (0.05-3.6mg) given on C1 Day (D) 1 and the target dose (0.15-132mg) given on C1D8, and on D1 of each subsequent cycle.
Results: At cut-off (April 13, 2020), 51 pts (median age: 62.0 years [range: 33-80]; high-risk [HR] cytogenetics [1q21, t(4;14), t(14;16), or del(17p)]: 28 pts) had been enrolled into Arm A. Median number of prior lines of therapy was 6 (range: 2-15). Prior treatments included: proteasome inhibitors (PIs), 100% (94.1% refractory); immunomodulatory drugs (IMiDs), 100% (98.0% refractory); anti-CD38 mAbs, 78.4% (92.5% refractory); autologous stem cell transplant, 86.3%. Overall, 66.7% of pts were triple-class refractory (≥1 PI, ≥1 IMiD, and ≥1 anti-CD38 mAb), and 94.1% of pts were refractory to their last therapy.
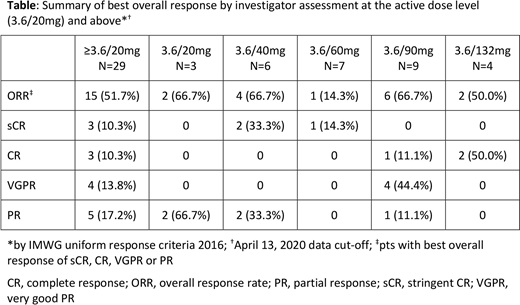
At cut-off, 46/51 pts were evaluable for efficacy. Responses were observed at the 3.6/20mg dose level and above, in 15/29 pts (51.7%) (Table). Responses included 3 stringent CRs, 3 CRs, 4 VGPRs, and 5 PRs (Table). At the 3.6/20mg dose level and above, responses were observed in pts with HR cytogenetics (9/17), triple-class refractory disease (10/20), and prior exposure to anti-CD38 mAbs (11/22), CAR-Ts (2/3), or ADCs (2/2). Duration of response data are evolving, with 6/15 pts in response for >6 months at cut-off.
Median follow-up for safety was 6.2 months (range: 0.2-26.3 months). Almost all pts (49/51) had ≥1 treatment-related AE. The most common treatment-related AE was CRS (Lee et al. 2014 criteria; 38/51 pts, 74.5%). CRS was Grade (Gr) 1 in 20 pts (39.2%), Gr 2 in 17 pts (33.3%), and Gr 3 in 1 pt (2%) (due to Gr 4 transaminase elevation). CRS was most common in C1 (38 pts) and was uncommon or absent in subsequent cycles (4 pts). Most CRS events (49/58, 84.5%) resolved within 2 days. 18/38 (47.3%) pts with CRS received tocilizumab and/or steroids. Other treatment-related AEs in ≥5 pts were neutropenia and lymphocyte count decreased (6 pts each, 11.8%), aspartate aminotransferase increased and platelet count decreased (5 pts each, 9.8%). Treatment-related Gr 3-4 AEs (20 pts, 39.2%) in ≥3 pts were lymphocyte count decreased (6 pts, 11.8%), neutropenia (5 pts, 9.8%), anemia and platelet count decreased (3 pts each, 5.9%). No treatment-related Gr 5 (fatal) AEs were observed. Treatment-related AEs leading to withdrawal of treatment were uncommon (1 pt, 2.0%). One DLT (Gr 3 pneumonia) was observed in the 3.6/90mg cohort, but the MTD was not reached.
BFCR4350A PK was linear across the active dose levels tested and the estimated half-life was supportive of the Q3W dosing regimen.
Conclusions: BFCR4350A monotherapy demonstrates promising activity in heavily pre-treated R/R MM, with deep and durable responses observed in pts with HR cytogenetics, triple-class refractory disease, and/or prior exposure to anti-CD38 mAbs, CAR-Ts, or ADCs. Toxicity was manageable, with C1 single step-up dosing effectively mitigating the risk for severe CRS and allowing escalation to clinically active doses. Updated data will be presented.
Cohen:Novartis: Other: Patents/Intellectual property licensed, Research Funding; Bristol-Myers Squibb: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Takeda,: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; GlaxoSmithKline: Membership on an entity's Board of Directors or advisory committees; Kite Pharma: Membership on an entity's Board of Directors or advisory committees; Oncopeptides: Membership on an entity's Board of Directors or advisory committees; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Genentech/Roche: Membership on an entity's Board of Directors or advisory committees. Harrison:Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; GSK: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; F. Hoffmann-La Roche: Consultancy, Honoraria; Novartis: Consultancy, Honoraria, Patents & Royalties: wrt panobinostat; BMS: Consultancy, Honoraria; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Haemalogix: Consultancy; Janssen: Honoraria; CRISPR Therapeutics: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen-Cilag: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Krishnan:Sutro: Membership on an entity's Board of Directors or advisory committees; Z Predicta: Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy; Regeneron: Consultancy; Takeda: Speakers Bureau; Amgen: Speakers Bureau; BMS/Celgene: Consultancy, Other: Stock BMS, Speakers Bureau; Sanofi: Consultancy. Fonseca:Amgen: Consultancy; BMS: Consultancy; Celgene: Consultancy; Takeda: Consultancy; Bayer: Consultancy; Janssen: Consultancy; Novartis: Consultancy; Pharmacyclics: Consultancy; Sanofi: Consultancy; Merck: Consultancy; Juno: Consultancy; Kite: Consultancy; Aduro: Consultancy; OncoTracker: Consultancy, Membership on an entity's Board of Directors or advisory committees; Oncopeptides: Consultancy; GSK: Consultancy; AbbVie: Consultancy; Adaptive Biotechnologies: Membership on an entity's Board of Directors or advisory committees. Forsberg:Celgene: Speakers Bureau; Genentech, Inc., Sanofi, Karyopharm, Abbvie: Research Funding. Spencer:AbbVie, Celgene, Haemalogix, Janssen, Sanofi, SecuraBio, Specialised Therapeutics Australia, Servier and Takeda: Consultancy; Amgen, Celgene, Haemalogix, Janssen, Servier and Takeda: Research Funding; AbbVie, Amgen, Celgene, Haemalogix, Janssen, Sanofi, SecuraBio, Specialised Therapeutics Australia, Servier and Takeda: Honoraria; Celgene, Janssen and Takeda: Speakers Bureau. Berdeja:BMS: Consultancy, Research Funding; Glenmark: Research Funding; Genentech, Inc.: Research Funding; Bioclinica: Consultancy; Teva: Research Funding; Vivolux: Research Funding; Abbvie: Research Funding; Cellularity: Research Funding; Acetylon: Research Funding; CURIS: Research Funding; Legend: Consultancy; Lilly: Research Funding; Constellation: Research Funding; EMD Sorono: Research Funding; Celgene: Consultancy, Research Funding; Novartis: Research Funding; Janssen: Consultancy, Research Funding; Prothena: Consultancy; Poseida: Research Funding; Amgen: Consultancy, Research Funding; Servier: Consultancy; Takeda: Consultancy, Research Funding; Bluebird: Research Funding; Karyopharm: Consultancy; Kite Pharma: Consultancy; CRISPR Therapeutics: Consultancy, Research Funding; Kesios: Research Funding. Li:Genentech, Inc./ F. Hoffmann-La Roche: Current Employment. Choeurng:Genentech, Inc.: Current Employment, Current equity holder in publicly-traded company. Vaze:Genentech, Inc./ F. Hoffmann-La Roche: Current Employment, Current equity holder in publicly-traded company. Samineni:Genentech, Inc.: Current Employment, Current equity holder in publicly-traded company. Sumiyoshi:Genentech, Inc.: Current Employment, Current equity holder in publicly-traded company, Divested equity in a private or publicly-traded company in the past 24 months. Cooper:Genentech, Inc./ F. Hoffmann-La Roche: Current Employment, Current equity holder in publicly-traded company. Fine:Genentech, Inc.: Current Employment; F. Hoffmann-La Roche: Current equity holder in publicly-traded company. Trudel:Janssen: Honoraria, Research Funding; Sanofi: Honoraria; GSK: Consultancy, Honoraria, Research Funding; Pfizer: Honoraria, Research Funding; Karyopharm: Honoraria; AstraZeneca: Honoraria; BMS: Consultancy, Honoraria, Research Funding; Genentech, Inc.: Research Funding; Amgen: Consultancy, Research Funding; Takeda: Honoraria.
BFCR4350A is a humanized IgG-based T-cell-engaging bispecific antibody that targets the most membrane-proximal domain of FcRH5 on myeloma cells and CD3 on T cells. Dual binding facilitates efficient immunological synapse formation, resulting in T-cell activation and killing of myeloma cells. BFCR4350A is an investigational agent.
This icon denotes a clinically relevant abstract

