

Introduction: Sickle cell disorders (SCD) is associated with progressive dysfunction of vital organs, including the cardiovascular system. While the development of pulmonary hypertension and left ventricular dysfunction have been previously studied, the burden of arrhythmias in SCD patients remains largely unknown. Thus, we aim to describe and analyze the prevalence and impact of arrhythmias in hospitalized adult patients with SCD and their impact in patient-oriented outcomes.
Methods: We identified incident arrhythmias in patients with SCD in the National Inpatient Sample (NIS) database in 2 years (2016-2017), using ICD-10 codes. We compared major patient characteristics, outcomes, and economic impact between groups of SCD patients with and without documented arrhythmias. A logistic regression model was used to control for age, sex, race, admission type, hospital characteristics, and relevant comorbidities. To increase statistical robustness, propensity-score matching for age, sex, income, and comorbidities was used to match 1144 SCD patients with arrhythmia and 1144 patients without.
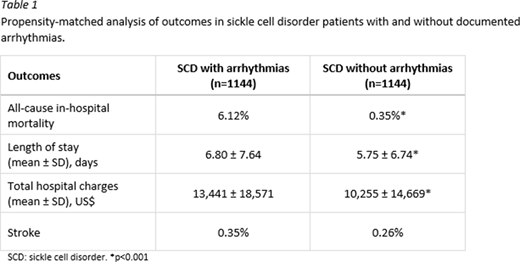
Results: Among inpatients with SCD in the database, 5,930 of 174,450 patients with SCD had documented arrhythmias (3.4%). The arrhythmia group consisted mostly of patients' sickle cell disease (5,650; 95%), while 245 had sickle cell trait, and 35 were classified as having other sickle cell disorders. Individuals in the arrhythmia group were significantly older (mean age 41.3, SD 14.1) than those with no arrhythmia (mean age 31.5, SD 10.3). Further, arrhythmia group had higher prevalence of hypertension (44.2% vs 19.1%, p<0.001), congestive heart failure (25.8% vs 4.1%, p<0.001), chronic kidney disease (24.0% vs 5.6%, p<0.001), valvular heart disease (9.3% vs 1.5%, p<0.001), myocardial infarction (4.1% vs 1.25%, p<0.001), type 2 diabetes mellitus (3.5% vs 1.7%, p<0.001), and pulmonary hypertension (3.5% vs 1.2%, p<0.001). When looking at major outcomes, after adjusting for confounders, arrhythmias were positively associated with all cause in-hospital mortality with an adjusted OR of 53.6 (95% CI 44.3, 65.1). After propensity-matching (Table 1), the arrhythmia group had a higher rate of all-cause in-hospital mortality (6.12% vs 0.35%, p<0.001), higher median length of stay (6.8 days vs 5.8 days, p<0.001), and mean total hospital charges ($13,441 vs $10,255, p<0.001). There was no statistically significant difference in the rate of stroke between both groups.
Conclusions: The presence of arrhythmias in patients with SCD was associated with markedly increased all cause in-hospital mortality, even after adjusting for confounders via logistic regression and propensity-score matching analyses. Despite a relatively low overall prevalence of 3.4% among this large inpatient cohort, this data suggests that arrhythmias may confer an important excess disease burden in SCD patients, including higher mortality. Intuitively, arrythmias confer higher mortality in patients with chronic disorders and multiple cardiovascular risks, whether this is specific to SCD deserves further study. Also, studies are needed to better understand the occurrence particularly in relation to active vaso-occlusive crisis and to evaluate whether SCD individuals with arrhythmias could potentially benefit from more intensive monitoring and/or better cardiovascular disease control.
No relevant conflicts of interest to declare.

