Key Points
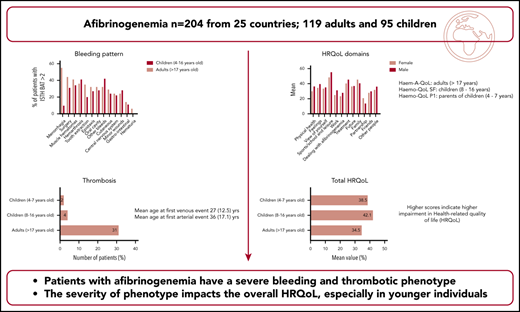
This international study on 204 patients with afibrinogenemia underlines the severity of bleeding and the frequency of thrombotic events.
The severity of clinical phenotype affects overall HRQoL, especially in younger patients.

Abstract
Due to the low prevalence of afibrinogenemia, epidemiologic data on afibrinogenemia are limited, and no data are available on health-related quality of life (HRQoL). We conducted a cross-sectional international study to characterize the clinical features, the fibrinogen supplementation modalities, and their impact on HRQoL in patients with afibrinogenemia. A total of 204 patients (119 adults and 85 children) from 25 countries were included. The bleeding phenotype was severe: 68 (33.3%) patients having at least one bleed per month and 48 (23%) a history of cerebral bleeding. About 35% (n = 72) of patients were treated with fibrinogen concentrates or cryoprecipitates as prophylaxis, 18.1% (n = 37) received ≥1 injection per week, and 16.6% (n = 34) were on home treatment. A thrombotic event was reported in venous and/or arterial territories by 37 (18.1%) patients. Thrombosis occurred even in young patients, and recurrence was frequent (7.4%). The total HRQoL was lower in children than in adults. Discomfort linked to treatment and limitations to sports and leisure were the main concerns. Women and children were particularly affected in family relationships. In multivariate analyses, younger age, residence in Asia or Africa, and a previous thrombotic event were statistically correlated with a worse HRQoL. In summary, our study underlines the severe bleeding and thrombotic phenotype and their impact on HRQoL in afibrinogenemia. The optimal strategy for fibrinogen supplementation needs to be determined. This trial was registered at www.clinicaltrials.gov as #NCT03484065.
Introduction
Congenital afibrinogenemia is a severe and rare coagulation disorder characterized by the complete absence of fibrinogen.1 Although important efforts have been made to understand the molecular physiopathology and to optimize the management of afibrinogenemia, the clinical epidemiology is still only partially documented.2 Bleeding is the principal symptom occurring in all tissues such as from the umbilical cord, skin, muscles, joints, and the central nervous system.3 Arterial and/or venous thrombosis is also a relatively common complication.4 An increased susceptibility to spontaneous splenic rupture, poor wound healing, and painful bone cysts are additional manifestations peculiar to afibrinogenemia.5 Fibrinogen supplementation is the keystone of management of bleeding in afibrinogenemia.6 Among the different available sources of fibrinogen, including fresh frozen plasma, cryoprecipitates, and fibrinogen concentrates; the concentrates provide the safer and more efficient option to treat bleeding and to prevent hemorrhagic complications.7 However, the optimal strategy of fibrinogen supplementation (on-demand vs prophylaxis) has not yet been established.8
Psychosocial factors and morbidity related to afibrinogenemia, as well as the necessity to have prompt access to fibrinogen supplementation, are likely to influence patients’ health-related quality of life (HRQoL). HRQoL is considered one of the most relevant clinical outcome assessments and is included as a primary or secondary end point in several clinical trials of coagulation disorders.9 Data on HRQoL in other rare bleeding disorders such as hemophilia or von Willebrand disease and immune thrombopenia are available,10-12 but there are no data on HRQoL in afibrinogenemia. Notably, it is unknown how the severity of the clinical phenotype and the fibrinogen supplementation affect the patient’s personal, professional, and social life, or whether the actual management truly reflects their preferences.
To fill these gaps, we conducted an international cross-sectional study aiming to assess the clinical epidemiology of afibrinogenemia, the fibrinogen supplementation modalities, and their impact on HRQoL.
Methods
Study population and data collection
An international cross-sectional study was conducted among centers involved in the care of patients with fibrinogen disorders. Centers were identified based on previous collaboration, ongoing collaborative projects, publications in the field, and a principal investigators’ network. All patients with afibrinogenemia aged >4 years were potentially eligible for enrollment in the study and were invited to participate. Afibrinogenemia was confirmed by the complete absence of fibrinogen, infinitely prolonged prothrombin and activated partial thromboplastin times, and, when genotype was available, a causative mutation in fibrinogen genes.1 All biological data were reviewed by the principal investigators (A.C., P.d.M.) who confirmed the diagnosis of afibrinogenemia. Patients were excluded if unable to understand the study documents. The protocol was approved by the institutional review board at each participating hospital in accordance with the Declaration of Helsinki. All patients (and/or parents in the case of minors) provided written informed consent before entering the study.
A standardized case report form was designed to assess demographic characteristics (age, sex, marital status, past pregnancies, employment, educational status, Social Security benefit, distance between home and the treatment center, and number of people in the household), usual bleeding treatment, current fibrinogen supplementation, history of hepatitis B or C and HIV, cardiovascular events, history of spontaneous spleen rupture, and bone cysts. The bleeding phenotype was assessed with the International Society on Thrombosis and Haemostasis Bleeding Assessment Tool (ISTH BAT).13 Referring clinicians completed the case report form based on their most recent medical files. Patients were invited for a follow-up visit if any information was outdated or incomplete.
Due to the rarity of afibrinogenemia, no disease-specific HRQoL questionnaire for these patients is available. We decided to use hemophilia-specific HRQoL instruments for the assessment of HRQoL because these questionnaires were available in all requested languages. We administered the Haemophilia Quality of Life Questionnaire for Adults (Haem-A-QoL; 46 items with 10 domains) to patients aged >17 years, the self-rated Haemophilia-Specific Quality of Life Assessment Instrument for Children and Adolescents Short Form (Haemo-QoL SF; 35 items with 9 domains) to children aged 8 to 16 years, and the proxy parent-rated Haemo-QoL Long Form PI (21 items with 8 domains) to parents of children aged 4 to 7 years.14,15 Participating patients were asked to come to the investigation site for a study visit. All patients were seen at least one time during the study period. Questionnaires were introduced by trained clinicians, and participants were asked to complete the questionnaires in the treatment center based on their experience in the previous 4 weeks. Answer categories ranged from “never” (1) to “all of the time” (5). The raw scores were transformed to a 0 to 100 scale, with higher scores indicating higher impairments in HRQoL.
Statistical methods
All variables recorded from participants were summarized as numbers and percentages for categorical variables and mean ± standard deviation for normally distributed continuous variables or median (quartile 1; quartile 3) for non-normally distributed variables. Groups were compared by using a χ2 test (binary variables) or Student t test (continuous variables). HRQoL values were transformed to a scale from 0 to 100 to compare the impairments across the different domains and to allow comparison across different age groups. Pearson’s correlation was used to determine the correlation between the HRQoL and the ISTH BAT and its 95% confidence interval according to the bootstrap method. Univariate linear regression models were performed to investigate the associations between the total score of the HRQoL and demographic and clinical data. Predefined variables (fibrinogen supplementation, age, sex, continent of residence, thrombotic phenotype, bleeding phenotype, and distance from the hemophilia center) were included in a multivariate linear model with the total score of HRQoL as dependent variable. A second model tested the modalities of fibrinogen supplementation (on-demand vs prophylaxis; on-demand vs prophylaxis <1 injection per week; on-demand vs prophylaxis ≥1 injection per week), adjusted for variables from previous model. All statistical tests were 2-sided, with a significance level of 0.05. All analyses were performed by using R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org).
Results
Biological and demographic characteristics
Between June 2016 and June 2019, a total of 211 patients from 46 treatment centers across 25 countries were enrolled (supplemental Table 1; supplemental Figure 2, available on the Blood Web site). Seven patients were excluded from the primary analyses due to incomplete clinical or HRQoL data. All patients had infinitely prolonged coagulation times and undetectable fibrinogen levels. Genotype was available for 69 patients (33.8%); most mutations were in the fibrinogen α chain, including the 11 kb recurrent large deletion (n = 12 [18.1%]) and the frameshift mutation c.510+1G>T (n = 7 [10.6%]) identified in each continent. In addition, most patients from Lebanon (n = 21 [65.6%]) were homozygous for a common nonsense mutation in FGA (c.635T>G). A list of all mutations is provided in supplemental Table 2.
Most patients were resident in Asia (n = 119 [58.3%]); others were from Europe (n = 39 [19.1%]), Africa (n = 39 [19.1%]), and the United States (n = 7 [3.4%]). Most patients were adults (58.3%), and 50.5% were male (Table 1). Patients were mainly diagnosed during the neonatal period, with a median age at diagnosis of 0.5 year (range, 0-28 years). Most adult patients were partnered/married and most had Social Security. One-third of adults had completed secondary education. At the time of inclusion, 20 (16.8%) adults were still students, and 74 (62.2%) were employed at least part-time. The median number of people per household was 5 (range, 0-11). About one-third of patients lived >100 km from a treatment center. Overall, 28 (13.7%) patients reported that at least 1 member of their family had died of afibrinogenemia.
Clinical features
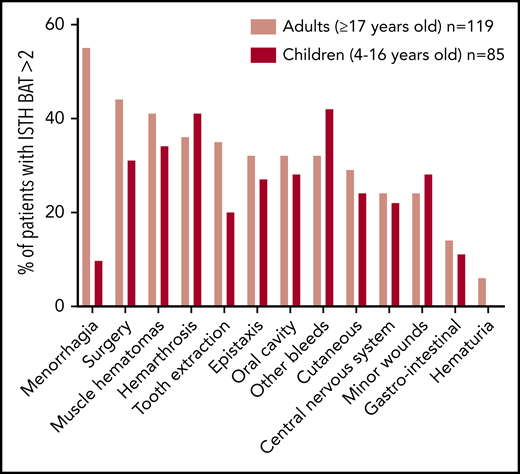
The bleeding phenotype was severe, with a median ISTH BAT score of 14 (Table 2). About one-third of patients reported at least one bleeding episode per month, even though 11 (5.4%) were asymptomatic. The severity of bleeding was also reflected by the high frequency of hemorrhages requiring a medical intervention (ISTH BAT score >2; n = 168 [82%]) as indicated in Figure 1. Perioperative bleeding (n = 82 [40%]), muscle hematomas, and hemarthrosis (each n = 78 [38%]) were particularly common. Overall, 48 patients (23%), including 19 children (22%), experienced central nervous system bleeding. Other bleeding, including umbilical stump bleeding, cephalohematoma, cheek hematoma, and excessive bleeding after venipuncture, were reported by 38 (32%) adults and 36 (42%) children. A majority of women (n = 42 [73.7%]) experienced heavy menstrual bleeding. All patients have received at least one blood product derivative and/or tranexamic acid as prophylaxis or management of acute bleeding. A few patients from Asia (n = 9 [7.5%]) and Africa (n = 7 [18%]) had no access to fibrinogen supplementation. Overall, 35.3% of patients were treated by regular prophylaxis, all by fibrinogen concentrate, with an increased proportion in younger children (43.5%); one-half of the prophylactically treated patients received >1 infusion per week and were on home treatment. Most patients under prophylaxis were residents of the United States (5 of 7 [71%]) and Europe (24 of 39 [62%]) compared with Asia (36 of 119 [30%]) and Africa (7 of 39 [18%]). The ISTH BAT score was neither statistically different between patients under prophylaxis and on-demand nor according to the frequency of bleeding.
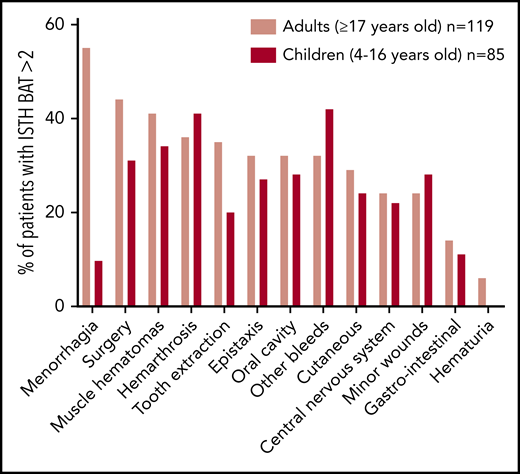
Pattern of bleeding in patients with afibrinogenemia according to age group. Values are expressed as percentage of patients experiencing bleeding requiring medical intervention (ISTH BAT score >2). Menorrhagia is expressed as percentage of women.
Pattern of bleeding in patients with afibrinogenemia according to age group. Values are expressed as percentage of patients experiencing bleeding requiring medical intervention (ISTH BAT score >2). Menorrhagia is expressed as percentage of women.
A total of 37 (18.1%) patients had experienced a thrombotic event; of these 37 patients, 16 (43.3%), 11 (29.7%), and 10 (27%) reported an event in venous, arterial, or both territories, respectively. Venous thromboses occurred in young patients with a mean age at first event of 27 years, including 6 children (7%). Arterial thromboses were also observed in young patients but only adults, with a mean age at first event of 36 years. Thrombotic recurrence occurred in 15 (40.5%) patients, in both venous (n = 6) and arterial (n = 9) territories. Four patients experienced multiple recurrences of acute peripheral ischemia of toes. Patients with venous thrombosis were mostly treated by using low-molecular-weight heparin (n = 13 [50%]), while a few received a direct oral anticoagulant (n = 4 [15.4%]) or a vitamin K antagonist (n = 4 [15.4%]). For arterial thromboses, 10 (47.7%) and 4 (19%) patients received aspirin and/or clopidogrel, respectively. Fifteen patients were under antithrombotic treatment at time of inclusion. Overall, data on antithrombotic treatment were missing for 7 patients.
The serologic status for hepatitis C and HIV was negative in 153 (75%) and 177 (86.8%) patients and unknown in 20 (9.8%) and 26 (12.7%) patients, respectively. Miscellaneous symptoms included spleen rupture in 11 (5.4%) patients and painful bone cysts in 36 (17.6%). Among the 27 women with a past pregnancy, 13 (48.1%) had one or more live births and 23 (85.1%) mentioned at least one fetal loss. Detailed data on successful pregnancies were not available.
Health-related quality of life
The mean HRQoL scores by domains and the total score are listed in Table 3. All age groups were particularly impaired in the domain “sports” (limitations to having sport) and the domain “treatment” (bothered by treatment). The third most affected domain in adults was “view of yourself” (impact of afibrinogenemia on yourself and your self-perception). The domains “partnership” and “dealing with afibrinogenemia” (personal adaptation to the disease) were those least affected. All children were greatly impaired in the dimension “family” (relationship with parents), whereas they reported a relatively satisfactory support by other kids and pleasant interaction with their friends (“other” and “friend” domains). Overall, men had a lower HRQoL for most domains compared with women. Adult women were more concerned in the “family” and “partnership” domains.
The ISTH BAT score was poorly correlated with total HRQoL (Pearson’s coefficient of correlation r = 0.15; 95% confidence interval, 0.01-0.28) (supplemental Figure 1). In univariate regression analyses (Table 4), the total HRQoL was better in Europe and the United States (n = 46) compared with Africa and Asia (n = 158) (P < .001). Availability of fibrinogen (fibrinogen concentrates or cryoprecipitates) was significantly associated with an improved total HRQoL, especially in children (P = .006). However, the modality of fibrinogen supplementation did not affect the total HRQoL. Adult patients who experienced a thrombotic event or were under an antithrombotic treatment had a statistically worse total HRQoL score (P = .006 and P = .040, respectively). No statistical differences in the total HRQoL were found for sex, obstetrical history (adult women only), ISTH BAT score (≥6 [n = 179] vs <6 [n = 26]), number of bleeding episodes per month, past cerebral bleeding, fibrinogen supplementation, location of administration (at home vs at the hospital), frequency of infusion (once a week vs more), living distance from treatment center, and presence of a bone cyst.
In a multivariate analysis model (Table 5), the place of residence, the thrombotic phenotype, the age (children), and the bleeding severity were independently associated with a poorer total HRQoL. When adjusted for these variables, the modality of fibrinogen supplementation (on-demand vs prophylaxis) and the frequency of prophylaxis (<1 or ≥1 injection per week) did not have an impact on total HRQoL.
Discussion
This international cohort is the largest comprising patients with afibrinogenemia and the first study describing patients’ HRQoL. Our results confirm the severe pattern of bleeding and the relative high prevalence of thrombotic events, even in young patients, with a negative impact on their HRQoL.
The bleeding phenotype of patients with afibrinogenemia is severe.16 Lak et al17 reported hemarthrosis (54%), muscle hematomas (72%), and cerebral bleeding (10%) in a historical Iranian cohort (n = 55). In the North American registry for rare bleeding disorders, all patients with afibrinogenemia (n = 7) experienced bleeding, mainly in skin (49%), musculoskeletal (26%), cranial (5%), and gastrointestinal (2%) hemorrhage.18 In the European Network of Rare Bleeding Disorders, >40% of patients with afibrinogenemia or hypofibrinogenemia had a history of grade III bleeding (defined as spontaneous major bleeding, including hematomas, hemarthrosis, central nervous bleeding, gastrointestinal, and umbilical cord bleeding). In a retrospective study including 100 patients with qualitative fibrinogen disorders (28 with hypofibrinogenemia), the mean annual incidence of bleeding episodes was estimated to be 0.5 for patients on prophylaxis and 0.7 for patients with on-demand therapy.19 We observed a similar bleeding pattern but a higher frequency of bleeding episodes. Indeed, in our series, most patients experienced at least one bleeding episode requiring a medical intervention, and one-third of patients reported at least one bleeding episode per month. Compared with the aforementioned study, we included only patients with afibrinogenemia, who present with a more severe phenotype than patients with hypofibrinogenemia. Even though the clinical features of afibrinogenemia are often very close to those of severe hypofibrinogenemia, patients presenting with the latter are still able to secrete a significant amount of fibrinogen in case of trauma and thus are less prone to spontaneous bleeding.20
The severity of bleeding in our cohort could also be related to the modalities of fibrinogen supplementation. However, our study, in which less than one-half of the patients were on prophylaxis, was not designed to compare strategies of fibrinogen supplementation. We observed a high frequency of surgery-related bleeding, supporting previous observations that surgery is a high-risk clinical situation in afibrinogenemia.19 Several clinical trials have reported the hemostatic efficacy of fibrinogen concentrate supplementation in patients with afibrinogenemia undergoing surgery.21,22 Our findings and recent data highlight the risk of bleeding in specific clinical settings and support the necessity of a specialized multidisciplinary approach for all patients with afibrinogenemia requiring an intervention.
Cerebral bleeding is the main cause of morbidity and mortality in afibrinogenemia.23 We observed a marked high prevalence of cerebral bleeding, similar to that reported by Sumitha et al24 in India. We were unable to assess whether these events were spontaneous or traumatic and related to specific cardiovascular risk factors such arterial hypertension. The high proportion of patients reporting such complications in our cohort reinforces the need for a clinical trial specifically aiming to assess the role of fibrinogen supplementation to prevent major bleeding since infancy.25 Secondary prophylaxis is usually considered after life-threatening bleeding and recurrent major bleeding.26 Data from randomized trials are lacking, although retrospective series of patients seem to suggest that the bleeding incidence is decreased in patients under prophylaxis compared with on-demand therapy.27,28 Only one-half of the patients under prophylaxis received treatment at home. Given that one-third lived far away from the treatment center, the importance of home prophylaxis, being potentially life-saving in case of sudden life-threatening bleeding, should be emphasized.
Thrombosis is a paradoxical complication of afibrinogenemia.29 In a systematic literature review, 48 reports of thromboembolisms in afibrinogenemia were analyzed, showing a wide range of venous and arterial thrombotic complications, also in unusual vascular territories.4 In our cohort, young patients experienced both venous and arterial thromboses, suggesting that the underlying pathogenesis of thrombosis in afibrinogenemia is complex.30 Elevated circulating levels of thrombin could play a major role. Indeed thrombin not entrapped by the fibrin clot is available, together with von Willebrand factor for platelet activation.31 Using an in vivo thrombosis model, Ni et al32 showed that the number of embolized thrombi was sixfold higher in fibrinogen knockout mice than in wild-type mice, with large emboli often leading to vessel occlusion. Fibrinogen supplementation has been advocated to increase the risk of thrombotic events.6 In our study, we were unable to determine an eventual time relationship with fibrinogen supplementation. It could be that an appropriate fibrinogen supplementation may, on the contrary, restore the hemostatic balance and therefore protect from the thrombotic risk.33 In view of this, the issue of thromboprophylaxis according to the bleeding risk, the fibrinogen supplementation strategy, and the personal and familial history should be addressed for all patients in high-risk thrombotic settings.34 Management of thrombosis is challenging because physicians have to deal with both the risk of bleeding related to the antithrombotic therapy and the risk of recurrent thrombosis. Vitamin K antagonists should be avoided because the monitoring of the international normalized ratio is not possible due to the spontaneously altered prothrombin time.35 Although low-molecular-weight heparin is the treatment of choice, emergent data highlight the potential safety and efficacy of direct oral anticoagulants in afibrinogenemia.36
Bone cysts were reported in 17.6% of patients. Their appearance is analogous to intraosseous pseudotumors observed in patients with hemophilia, although in afibrinogenemia, cysts are heterogeneous in terms of the extent, location, and different stages of the underlying intraosseous hemorrhages.37 The distribution of hemorrhages along the trabeculae fitting to the lines of stress suggest that they could be triggered by mechanical forces.38 Excessive thrombin could also be a cause, as thrombin stimulates production of osteoclastogenic factors by osteoblastic cells and inhibits the early stages of osteoclast differentiation.39 Prevalence of bone cysts is likely to be underdiagnosed. Magnetic resonance imaging should be discussed in patients reporting rheumatic pains, and the benefit of fibrinogen supplementation in relieving pain should be further investigated.
Pregnancy is a very high-risk clinical situation. Indeed, fibrinogen plays several fundamental roles during pregnancy, including the support of early-term trophoblast proliferation,40 the spreading and maintaining of the placenta,41 and the development of the feto-maternal circulation.42 In that setting, early fibrinogen supplementation is mandatory in afibrinogenemia.43 All successful pregnancies in our cohort were performed under fibrinogen supplementation. On the contrary, several recurrent miscarriages resulted from the absence or insufficient availability of fibrinogen supplementation.
Surprisingly, HRQoL in patients with afibrinogenemia was relatively satisfactory in most domains of the Haemo-QoL (pediatric patients) or Haem-A-QoL (adult patients). Obviously, we cannot make a direct comparison with studies of HRQoL in patients with severe hemophilia, but some similitudes can be pointed out. For instance, in both diseases, adults seemed to be mainly affected in the domain “Sports & leisure,” which can be explained by limitations in sports activities due to their physical health,44 whereas children are particularly concerned by the domain “family,” which can be related to overprotection by parents.45 The clinical phenotype partially influenced the HRQoL. The severity of bleeding, as assessed by using the ISTH BAT score and the frequency of bleeding, did not have a significant impact on total HRQoL. However, heavy menstrual bleeding was a common symptom with a probable adverse effect on women’s HRQoL. We can speculate that heavy menstrual bleeding led to limitations in daily activities and changes in social functioning, as suggested by the impaired “partnership” subdomain in adult women in our study. The thrombotic phenotype had a significantly negative impact on HRQoL. It is likely that patients with thrombosis, in addition to their anxiety related to the increased bleeding tendency due to antithrombotic therapy and their worries of recurrent thrombosis, have more hospitalizations, and need a closer follow-up. The modality of fibrinogen supplementation (ie, prophylaxis vs on-demand) does not seem to affect the HRQoL of patients. However, our study reflects only patients more recent perceptions (last weeks) and does not take into account an eventual improvement of HRQoL following prior initiation of prophylaxis. The continent of residence was one of the main factors influencing the HRQoL. We anticipated that cultural considerations would influence the feeling and perception of patients. In some countries, a patient’s relevant outcome is to be able to participate in activities of daily life, whereas in others, the goals include survival, the absence of spontaneous bleeding, and getting appropriate fibrinogen supplementation.
Our study has several limitations. The study design did not allow us to determine directly the impact of fibrinogen supplementation on the clinical phenotype. Notably, as the time when fibrinogen prophylaxis started was not determined, its overall impact on the ISTH BAT score and HRQoL could be underestimated. However, we describe the real-life picture of modality and frequency of fibrinogen supplementation in a large cohort of patients with afibrinogenemia. The ongoing prospective registry PRORBDD (http://eu.rbdd.org, last accessed 7 July 2020) will hopefully reinforce our observations and offer insights on the role of prophylaxis vs an on-demand regimen therapy in afibrinogenemia. The severity of the bleeding phenotype was variable among our patients. We did not analyze the presence of genetic modifiers (eg, rare mutations or common polymorphisms in other genes of the coagulation or fibrinolytic pathways), which could contribute to explaining the heterogeneous clinical phenotype. The future interest in such patients will be to assess a larger fraction of the genome, to try to have prognostic information, and if possible, to tailor the therapy/prophylaxis. The HRQoL questionnaires used were not designed and validated for afibrinogenemia. The Haemo-QoL and Haem-A-QoL questionnaires used here were originally developed for patients with hemophilia, with items not fully adapted to women and partially focused on arthropathy, which is a less invalidating complication in afibrinogenemia. The benefit of using these hemophilia-specific instruments was their availability in almost all languages of the participating countries. Additional efforts should be made to offer a specific HRQoL questionnaire for patients experiencing rare bleeding disorders, taking aspects such as heavy menstrual bleeding into account. Indeed, we did not administer a menorrhagia-specific HRQoL instrument, which would have helped to further assess the specific problems of these women. The ISTH BAT is a widely used tool to assess severity of bleeding. However, it has not been specifically developed for afibrinogenemia, and its sensitivity in that context can be questioned. Establishment of individual specific bleeding tools with correction factors for sex and age is the next challenge.
In summary, we found that bleeding and thrombotic phenotype are severe, even in young patients with afibrinogenemia. The clinical phenotype significantly affects the HRQoL, especially in children regarding limitations in sports and leisure as well as family relationships. International collaborations such as ours offer the opportunity to gather more clinical and biological data, improving our knowledge of such a rare disease and ultimately highlighting the patients’ treatment preferences.
For original data, please contact Alessandro Casini (alessandro.casini@hcuge.ch).
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors thank all collaborators, nurses, and physicians who contributed to the realization of the study. The authors warmly thank Philippe Halban for the critical review of the manuscript.
Authorship
Contribution: A.C., C.D.K., C.S., F.P., M.A., P.d.M., and S.v.M. designed the study, performed research, and wrote the manuscript; A.C. and P.d.M. wrote the manuscript and performed analyses; S.v.M. provided the HRQoL questionnaires and interpreted the HRQoL data; A.C., F.P., P.d.M., and S.v.M. contributed expert review; and all authors contributed data and performed research.
Conflict-of-interest disclosure: A.C. reports grants and fees paid to his institution from CSL Behring, Octapharma, Sobi, Shire, Takeda, and Novo Nordisk. P.d.M. has received grants and fees from Bayer, CSL Behring, LFB, Novo Nordisk, Octapharma, and Shire. The remaining authors declare no competing financial interests.
All members of the QualyAfib Study Group contributed to patient inclusion and are listed in supplemental Table 3.
Correspondence: Alessandro Casini, Division of Angiology and Hemostasis, University Hospitals of Geneva, 1211 Geneva 14, Switzerland; e-mail: alessandro.casini@hcuge.ch.