

Abstract
Abstract 4193
The management of red cell disorders especially Thalassaemias is a fine balance between adequate transfusion and maintainence of Ferritin levels within a threshold. To achieve this, UK thalassaemia guidelines advice :
Pretransfusion Haemoglobin (Hb) 9.5-10grams/dl
Ferritin levels <1500 ug/lit.
Splenectomy if transfusion requirements > 200mls/kg/year.
Is a retrospective audit to check if the above standards are met. The study period was 1 year (Jan –Dec 2008) ;the cohort being 12 patients(ages ranging from 22 to 46),10 with Beta thalassaemia major, 1 thalassaemia intermedia and 1 with erythropoietic porphyria.
1.pretransfusion Hb
64%transfusions had a mean pretransfusion Hb>10.
2. Mean Ferritin levels :
| Ferritin levels | Number of patients |
|---|---|
| < 1500 | 3 |
| 1500 – 2500 | 3 |
| 2500 to 3500 | 1 |
| 3500 – 6000 | 3 |
| > 6000 | 2 |
| Ferritin levels | Number of patients |
|---|---|
| < 1500 | 3 |
| 1500 – 2500 | 3 |
| 2500 to 3500 | 1 |
| 3500 – 6000 | 3 |
| > 6000 | 2 |
75%patients had Ferritin levels>1500.
3 patients: had cardiac + liver iron overload & ferritin>5000, were initially on Deferasirox, but later swapped to desferol and deferiprone combination based on MR T2*results.
3 patient s : had cardic and liver iron overload -2 had associated endocrine dysfunction with Ferritins >2000;the first was already on Desferol, Deferiprone was added to this. The second was on Desferol +Deferiprone combination with little response, was changed to Deferasirox increased upto 30 mg/kg, however the Ferritin levels showed a progressive rise and patient was considered for trial (Deferasirox40 mg/kg Vs Desferol). 1 patient had a Ferritin<1500 on Deferasirox, and continued the same.
3 Patients : had neither cardiac or liver iron overload, but had endocrine dysfunction.2 of them had Ferritins around 1500 and were on Deferasirox which was continued .The third patient stopped Deferasirox when Ferritin dipped<500,and restarted at a lower dose(from 20 mg to 10 mg/kg) when the Ferritin levels crept up to >800.
2 patients: had liver iron overload, no cardiac overload, 1st patient having a ferritin <1500, on Deferasirox and continued on the same. The second had Ferritin >5000, hypersplenism (spleen 19 cms on ultrasound)frequent transfusion requirements(>330 mls/kg/year) and pancytopenia on Desferol was considered for Splenectomy.
1patient: with clostrophobia was reluctant to undergo MR scanning, was commenced on Desferol + Deferoprone combination based on ferritin levels>4000.
UK NATIONAL GUIDELINES FOR MANAGEMENT OF IRON OVERLOAD
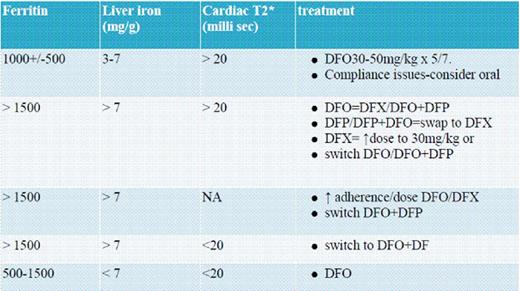
DFO = Desferol, DFX = Deferasirox, DFP = Deferiprone
Monitoring: All patients had monthly complete blood count,liver, kidney and endocrine function tests; and annual MR T2* imaging of heart / liver and ophthalmology and audiology assesments. Those with cardiac iron overload had cardiology followup .Those with liver iron overload had annual alphafetoprotein levels and Liver ultrasound.
3.Splenectomy : 42%(5/12)patients had a transfusion requirement of >200mls/kg/year.
Of the 12 patients:1 had regular 3 weekly transfusions,regardless of the Hb;3 patients were transfused on prewritten regimes designed at least 2 years earlier and lacked modification to current iron status.8 patients were transfused on a symptomatic basis-the most common symptom being ‘tiredness’-2 had left ventricular ejection fraction<50%,1 chronic fatigue syndrome,3 insulin dependant diabetes with high HBA1c levels,1 had hypocalcemia with a subsequent diagnosisof Hypoparathyroidism ; and 1 patient had sexual dysfunction with some improvement post transfusion. Clearly all 8 patients had other causes attributable to their ‘tiredness’.
Treatment allocation / monitoring was100% in keeping with guidelines,but the incidence of cardiac / liver iron overload in 66% and Ferritin levels >1500 in 75% of the patients could be improved by :strictly adhering to pretransfusion Hbs 9 to 10.5,reviewing prewritten transfusion regimes in the context of current iron overload,careful exclusion of other causes of symptoms ;avoiding transfusing patients purely on a 3 / 4 weekly basis .Lastly Splenectomy needs consideration in those with transfusion requirments>200mls/kg/yr.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal