

Abstract
Abstract 1260
Although the efficacy of cord blood transplantation (CBT) from unrelated donors as viable alternative for patients in need of hemtopoietic stem cell transplantation (HSCT) is supported by growing evidences, viral infections related to delayed immune reconstitution remains important problems for further improvement of clinical outcomes. To evaluate incidences and outcomes of late viral infections after CBT by comparison with those after unrelated bone marrow transplantation (uBMT), we retrospectively analyzed the records of 281 Japanese adult patients who underwent allogeneic unrelated HSCT for the first time at the Toranomon Hospital between January, 2002 and March, 2010, and who survived more than 100 days after HSCT without the lost-to-follow-up or retransplantation before day 100. Between 50 days and 5 years after HSCT, 116 patients had at least one late infectious episode with a cumulative incidence of 52.2%, at a median of 157 (50-1597) days after HSCT. The 5-year cumulative incidence of any late viral infections was greater in CBT versus uBMT recipients (60.7% vs. 42.2%, respectively; P=0.039, Figure 1). Thirty-three patients (28.4%) had 2 or more episodes caused by different viruses, and a total of 152 late infectious episodes were documented. The median onset of the episodes was similar between the both groups (median onset 226 days vs 222 days, P=0.89). The most common late viral infection is varicella-zoster virus (VZV) reactivation, accounting for 28.8% (disseminated 10, localized 34), followed by hemorrhagic cystitis associated with adeno- and/or BK viruria (28.2%), cytomegalovirus (CMV) diseases (16.4%; gastrointestinal diseases 23, retinitis 1, pneumonia 1), and respiratory tract infections caused by influenza virus, parainfluenza virus or respiratory syncytial virus (15.8%; upper 26, lower 8), and Epstein-barr virus lymphoproliferative diseases (4.6%). The remaining 10 infectious episodes were caused by relatively rare type of viruses including herpes simplex virus, JC virus, measles virus, mumps virus, norovirus and parvovirus, all of which occurred only in CBT recipients. Of all these viral infections, only VZV reactivation developed significantly more frequent in CBT than in uBMT recipients (P=34.0% vs 17.0%, P=0.023). There was no difference of dissemination rate between the both groups, and all the patients responded well to treatment with antiviral agents. The late viral infection was a primary cause of death in 3 episodes, all of which were pneumonia caused by CMV, influenza virus and parainfluenza virus. The 5-year incidence of infection-related mortality did not differ between CBT and uBMT recipients (0.7% vs 3.1%, P=0.46). Non-relapse mortality occurred in 11.8 % and 16.4 % patients in the CBT and uBMT groups (P=0.71). These findings suggested that cord blood might be as an acceptable and useful stem-cell source as bone marrow from unrelated donors in terms of risks of viral infection in the late posttransplant period.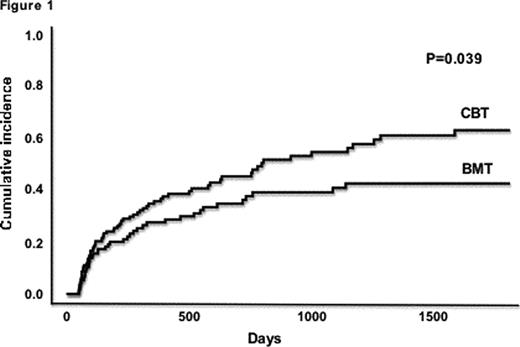

Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal