

Abstract
Abstract 171
The BABY HUG trial was a multi-center double-blinded randomized comparison of hydroxyurea (HU) versus placebo in infants (mean age 13.6 mo. at entry) with HbSS/Sβ° thalassemia who were followed for 2 years [Lancet 377(2011):1663–1672; Clinical Trials #NCT00006400]. Hydroxyurea therapy was associated with less pain, dactylitis, acute chest syndrome (ACS), hospitalization (HSN), and transfusion (TX) and with improved hematologic values; toxicity was limited to mild-moderate neutropenia. On the basis of the safety and efficacy data from this trial, it was concluded that hydroxyurea therapy can be considered for all very young children with sickle cell anemia (SCA). With anticipated broader use of hydroxyurea in this population, we examined estimated medical costs of care (based on Medicaid reimbursement) in treated versus placebo subjects.
The BABY HUG database (C-TASC, Baltimore, MD) was utilized to compare inpatient events in subjects receiving hydroxyurea with those receiving placebo. Unit costs were estimated from the 2009 Thomson Reuters MarketScan® Multi-state Medicaid Database for children with HbSS (ICD-9 codes 282.61 or 282.62), ages 1–3 years. Inpatient costs included emergency department (ED) costs for admissions from an ED in about 80% of the 748 admissions in the database. Inpatient cost estimates were based on length of stay (LOS) modified by a diagnosis of ACS or splenic sequestration (SpS) or a procedure code for a TX. Outpatient expenses were estimated based on the schedule required for BABY HUG (and recommended for clinical use) and a “standard” schedule for 1–3 year-olds with SCA based on management protocols at 3 pediatric sickle cell centers in the US.
96 subjects were randomized to hydroxyurea (83 completed the trial); 97 received placebo (84 completed the trial). In the full study, there were 232 hospitalizations (for any cause) in those receiving hydroxyurea and 324 in those on placebo; inpatient data were captured for only the final 77% of admissions (between 2/06 and 9/09). The LOS for subjects receiving hydroxyurea (mean 3.7, median 3, range 1–9 days) did not differ from those receiving placebo (3.6, 3, 1–13). Estimated inpatient and outpatient costs are shown in Tables 1 and 2.
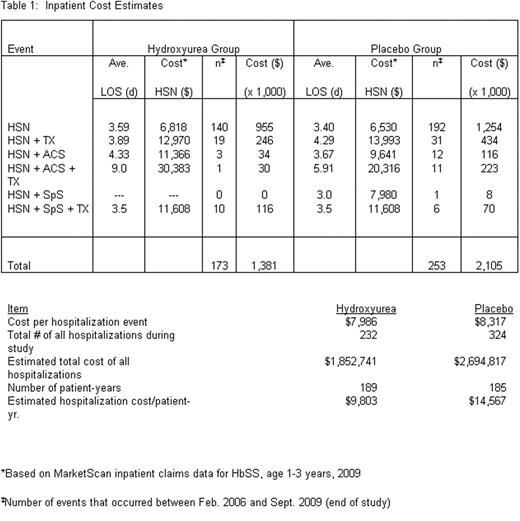
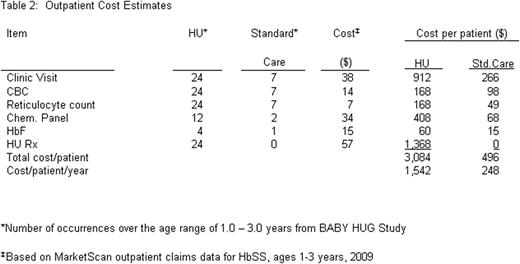
When inpatient and outpatient expenses were combined, the annual cost for 1–3 year-old children with SCA was $11,345 on hydroxyurea and $14,815 on placebo, a difference of $3,470.
Despite increased outpatient care expenses from clinic visits, laboratory monitoring, and hydroxyurea, savings on inpatient care resulted in an overall reduction in estimated annual per patient expenditure of approximately 23%. A limitation of our analysis was the dependence on MarketScan Medicaid data in lieu of the availability of specific expenses of the subjects participating in the BABY HUG study. Medicaid data may understate costs of care; based on prior analyses, we estimate that costs to private payers may be 20–30% greater than Medicaid reimbursements. We conclude that increased use of hydroxyurea treatment in children with SCA can lead to significant medical cost savings.
Off Label Use: Hydroxyurea is not indicated for treatment of children with sickle cell disease. Use of this medication was for clinical indications and not mandated by this observational study.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal