

Abstract
Abstract 2123
Little is known about the relative rate of pubertal development among children with different phenotypes of sickle cell disease (SCD). This study proposes, for the first time, to compare the influence of SCD phenotypes on pubertal development (PD) and body mass. We hypothesized that differences in pubertal development and body mass index (BMI) are modulated by SCD phenotype and treatment modality.
We therefore conducted a cross-sectional study of SCD children and adolescents aged 8 – 18 years old (yo) to determine the impact of SCD phenotype and treatments on pubertal development (according to sexual maturity rating by Tanner stages, TS) and BMI. Participants were recruited from Children's Healthcare of Atlanta and enrolled after written informed consent was obtained. Subjects' age, height, weight, self-reported TS (via questionnaire), physician-reported TS, and major therapies were recorded. We investigated two major phenotypes, hemoglobin SC disease (SC, n= 16) and sickle cell anemia (SS, n=58). Within the SS group there were three treatment sub-groups, no-treatment (SS, n=18), hydroxyurea (S HU, n=21), and red blood cell transfusion (S Tx, n=19). Since age is associated with achieving a certain level of sexual maturity we divided the participants according to Nelson's Textbook of Pediatrics. A Tanner stage of <3 in mid adolescence (14–16 yo) or <5 in late adolescence (17–18 yo) indicates delayed PD. Participants' BMIs were placed in weight status categories according to CDC standards as follows: underweight (<5th percentile), normal weight (5– 85th percentile), and overweight/ obese (85–95th/ above 95th percentile). Results were corrected for gender and a non-parametric Mann-Whitney test was used to compare means.
Early adolescent (10–13 yo) SS females had significantly lower self-reported TS, than those with SC (2±1 vs.3±1, means±SD respectively, p=0.018) or S Tx (3±0, p=0.031). Mid adolescent S HU females had significantly lower self-reported TS than SS (3±1 vs. 5±1, p=0.027) or SC (5±0, p=0.034), reflecting more past SCD complications in the S HU group. One late adolescent male in the Hb S Tx group did not attain Tanner 5. Across all groups, more than 50% of the remaining participants achieved normal PD (Table 1). Investigating BMI (kg/M2) by developmental stages revealed that early adolescent SC females had significantly higher BMI than S HU (23±9 vs. 16±1, p=0.036) and SS females (15±1, p=0.028). For early adolescent S Tx males, BMI was significantly higher than S HU males (19±1 vs.16±1, p=0.034). SS children were more likely than SC to be underweight (11–14%) regardless of treatment, and least likely to be overweight with no treatment (Table 2).
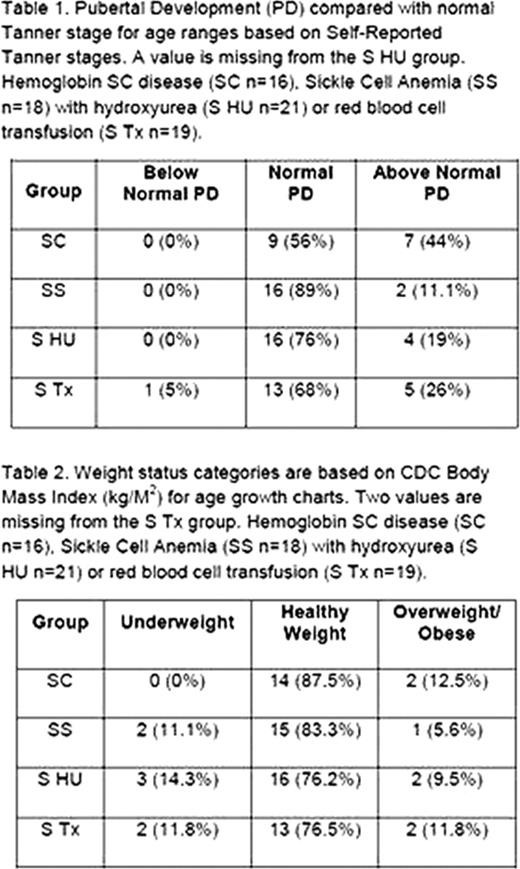
These results show that there are differences in level of maturity and BMI based on SCD phenotype and treatment modality. Differences seen in treatments are possibly due to the length of time on treatment modality prior to enrolling in study. Although these differences exist, the majority of participants lie within the normal PD range. Surprisingly, sickle cell disease, which is usually associated with delayed development, did not affect the ability of most these children to reach puberty within the expected timeframe. However, they still experienced lower than normal body mass. Lower BMI and slower puberty may be related to the number and severity of SCD complications, rather than hemoglobin phenotype alone. More studies are needed to better understand the effects of SCD severity and diet on somatic growth and puberty.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal