

Abstract
Abstract 2837
Rai and Binet staging systems are not devoid of some limitations, including the lack of evaluation of thoracic and abdominal lymphadenopathies. The widely-used IWCLL guidelines do not incorporate use of TB-CT scan in the diagnostic algorithm. In the present study, we investigated whether TB-CT scans could up-stage Binet stage A CLL patients included in the prospective multicenter O-CLL01 GISL study (clinicaltrial.gov ID: NCT00917549), and whether this subgroup presented differences in prognostic markers and in progression-free survival (PFS). To date, 454 patients have been enrolled and TB-CT scans were available in 238 patients. The median age was 60 years (range, 33–71) and 136 (57%) were male. According to Rai, 180 patients were at low risk (stage 0) and 58 at intermediate risk (stages I-II). b2-microglobulin was elevated in 35.5% of cases. Seventy-eight patients (32%) were IgVH unmutated, 108 patients (45%) had a high ZAP-70 expression, 45 patients (19%) were CD38 positive (>30%). FISH data were available in 226/238 cases; the most frequent abnormality was del(13)(q14) (105 pts, 46.5%), followed by trisomy 12 (24 pts, 10.6%), del(11q22.3) (13 pts 5.5%), del(17p13) (4 pts 1.8%) while 80 cases (35.4%) cytogenetics were normal. Cytogenetic abnormalities were clustered in 3 risk groups [i.e. low (del(13q14) and normal), intermediate (trisomy 12) and high risk (del(11q22) and del(17p13)]. Two hundred six out of 238 patients had a minimum follow-up of 6 months and were evaluable for PFS. Considering TB-CT scan, 54 out of 238 analyzed (22.7%) patients converted into Binet stage B. Notably, 63% were male, b2-microglobulin was elevated in 50% of cases, 42.6% were IgVH unmutated, 48.1% had a high ZAP-70 expression, 27.8% were CD38 positive, and 17.6% showed a high-risk FISH. Binet B patients showed a statistically higher rate of cases with high risk cytogenetic abnormalities than Binet A patients (17.6% vs 4.6%; p=0.032). While, no statistically different distribution of gender, age, B2-microglobulin, IgVH mutational status, CD38 or ZAP-70 expression were observed between the two subgroups. After a median follow-up of 24 months 46/206 (22%) evaluable cases showed disease progression. Binet B patients showed a PFS significantly shorter than those with a normal TB-CT (2-years PFS probability, 85.6% vs 68.5%; p<0.0001). According to the Rai classification 102/180 (56.7%) low risk patients were re-defined as intermediate risk with the integration of TB-CT scan. This subset of patients showed a statistically higher rate of cases with elevated ZAP-70 (51.5% vs 35.9%; p=0.049) and CD38 (22.5% vs 10.3%; p=0.045) than patients at low risk. After a median follow-up of 25 months, 23/154 (15%) of evaluable cases showed disease progression. Patients with an intermediate risk Rai stage showed a PFS significantly shorter than those with a low risk (2-years PFS probability, 82% vs 96%; p=0.002). In this setting 70 cases met the diagnostic criteria of monoclonal B-lymphocytosis (<5 × 109/L B- lymphocytes in the blood). With the integration of TB-CT scan 30/70 (42.9%) monoclonal B-lymphocytosis patients were re-defined as intermediate risk according the Rai classification. No statistically different distribution of clinical and biological parameters were observed between cases who remained in the low risk stage and those who became at intermediate risk. After a median follow-up of 28 months 4/57 cases evaluable for PFS showed a disease progression (2 cases for each subgroup). Considering low risk Rai stage, no statistical difference in PFS was observed among nonCT-upstaged MBL, CT-upstaged MBL, nonCT-upstaged Rai 0, while CT-upstaged Rai 0 cases showed a statistically shorter PFS (p<.0001) than the other groups (Figure 1). Finally, TB-CT scan allowed the early identification of a second neoplasia in 2 cases (lung cancer 1 pt, renal cell carcinoma 1 pt). Our preliminary data indicate that the integration of TB-CT scans in the clinical staging allows for an effective clinical discrimination of Binet A CLL cases in approximately 23% of cases at more advanced stages, predicting a worse clinical outcome. However, the use of TB-CT scanning for upstaging is not beneficial for predicting PFS in MBL cases. A longer follow-up will demonstrate whether the inclusion of TB-CT scan in the initial work-up of patients with early-stage CLL will provide clinically relevant prognostic information.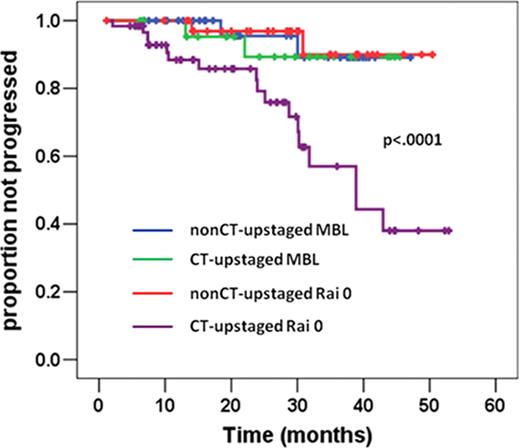
Figure 1.

PFS in Rai 0 cases.
Disclosures:
Di Raimondo:celgene: Honoraria. Foà:Bristol-Myers Squibb: Consultancy, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal