

Abstract
Abstract 3045
We have reported that measuring the activation markers and homing molecules on T-cells obtained from human peripheral blood (PB) samples provides useful information for predicting acute graft-versus-host disease (GVHD) severity in affected organs. Although T-cells are major player for developing GVHD, rodent GVHD studies have demonstrated that other immune cells such as monocytes/macrophages, B-cells, and mast cells involved in the pathogenesis of acute and chronic GVHD. We, therefore, evaluated activation markers and homing molecules regularly not only on T-cells but also on monocytes in PB obtained from 31 childhood patients (more than 600 samples at various time points) receiving hematopoietic stem cell transplantation (HSCT) by multicolor flow cytometry. The following markers were used: CD69, CD25, and HLA-DR for T cell activation, CCR4, CCR5, CXCR3, CCR9, and CLA for homing markers. Inflammatory monocytes were defined as CD14dimCD16+ cells or CD14+CD163+ cells. In addition we combined the data of cytokine profiles secreted mainly by T cells such as soluble interleukin 2 receptor, or monocytes such as neopterin, or both such as tumor necrosis factor-α (TNF-α), soluble TNF-αRI, and soluble TNF-αRII. In all cases showing acute GVHD, both T-cell and monocyte activation markers were elevated. Only either T-cell or monocyte activation was not observed in acute GVHD cases. However, we have some interesting results classified according to the status of T-cells and monocytes after day 100: 1) In the cases both T-cells and monocytes were highly activated as shown in Figure 1A, tapering of immunosuppressants led to exacerbation of GVHD, and prolonged administration of the drugs including steroids were needed. However steroid response itself was relatively good. 2) In the cases only T-cells, much less monocytes, were activated as shown in Figure 1B, calcineurin inhibitors were quite effective in improving GVHD. 3) In the cases of sustained chronic GVHD, neither T-cells nor mononytes were activated as shown in Figure 1C. Response to immunosuppressants was quite low. 4) When CD4 T-cell repertoire, not CD8, became normal, tapering of drugs was successful. In all cases successfully tapered immunosuppressive drugs, elevated activation markers of T-cells and monocytes completely returned to same levels of normal volunteers. In conclusion, evaluating the activation markers and homing molecules not only on T-cells but also on monocytes, combined with cytokine profiling, might provide useful information for management of patients with prolonged GVHD.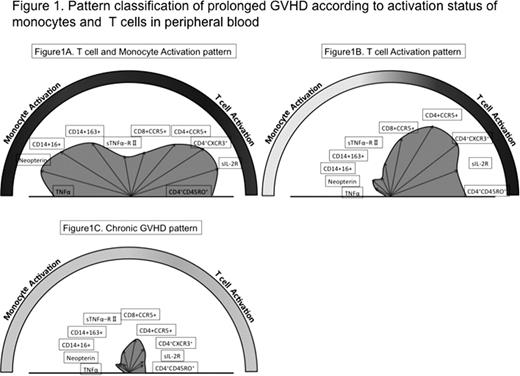

Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal