

Abstract
Abstract 4200
Neutropenia is a frequent complication of myelosuppressive chemotherapy. In the presence of fever or other evidence of infection, neutropenia typically necessitates inpatient care, although a minority of less severe episodes is treated on an outpatient basis or at home. While the cost of febrile neutropenia (FN) requiring hospitalization has been reported to be high in the United States, little is known about the cost of FN treated on an inpatient basis in other countries or the cost of FN treated in other settings.
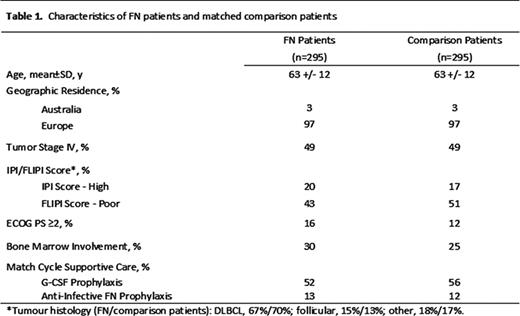
Data were obtained from an observational study of supportive care in patients with non-Hodgkin's lymphoma (n=1,829) receiving CHOP-14 or CHOP-21 chemotherapy (±rituximab) predominantly across Europe. FN was defined as a single oral temperature of ≥38.3°C or temperature of ≥38.0°C for ≥1 hour, and neutrophil count of <0.5×109/L or <1.0×109/L and predicted to fall below 0.5×109/L. Patients developing FN in a given cycle (“FN patients”), starting with the first cycle, were matched (1:1, without replacement) on age, tumor stage, chemotherapy, and other factors to those not developing FN in that cycle (“comparison patients”), irrespective of FN experience in subsequent cycles; matched pairs were stratified on the basis of the initial setting of care for FN (ie, inpatient, outpatient, home, and other/unknown). FN-related healthcare utilization and costs (estimated from UK National Health Service perspective [2010]) were tallied for patients from the match cycle through the last chemotherapy cycle (“follow-up”).
295 FN patients were matched to comparison patients; matched groups were similar in terms of baseline characteristics (Table 1). 76% of FN patients required inpatient care for the initial FN event; corresponding percentages for outpatient care and home care were 6% and 12%. Among FN patients requiring inpatient care, FN costs totaled \P9476 (95%CI \P8625-\P10418) versus \P2288 (\P1881-\P2705) for matched comparison patients, a difference of \P7188 (\P6339-\P8079); care subsequent to initial hospitalization accounted for \P1914 (or, 27%) of the higher FN costs (Table 2). Differences in costs between FN patients requiring outpatient care and home care, and their matched comparison patients, were \P1184 (\P-408-\P2996) and \P1638 (\P600-\P2805), respectively.
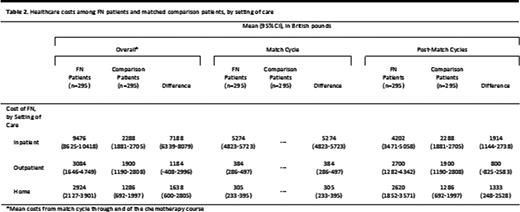
Cost of chemotherapy-induced FN requiring inpatient care among patients with non-Hodgkin's lymphoma in European clinical practice is substantial, and is comparable to the economic burden of FN in the US (US$11496 in this study vs US$12397 in the study by Weycker et al [Ann Oncol 2008]); follow-on care represents more than one-quarter of the total cost. Cost of FN requiring outpatient care and home care also is considerable.
Weycker:Amgen: Consultancy. Danel:Amgen: Employment, Equity Ownership. Bendall:Amgen (Europe) GmbH: Consultancy; Amgen UK: Consultancy. Lipsitz:Amgen: Consultancy. Pettengell:Amgen (Europe) GmbH: Honoraria; Roche: Honoraria; Celgene: Honoraria; Chugai: Honoraria; GSK: Honoraria; CTI: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal