

Abstract
Abstract 452 FN2
FN2
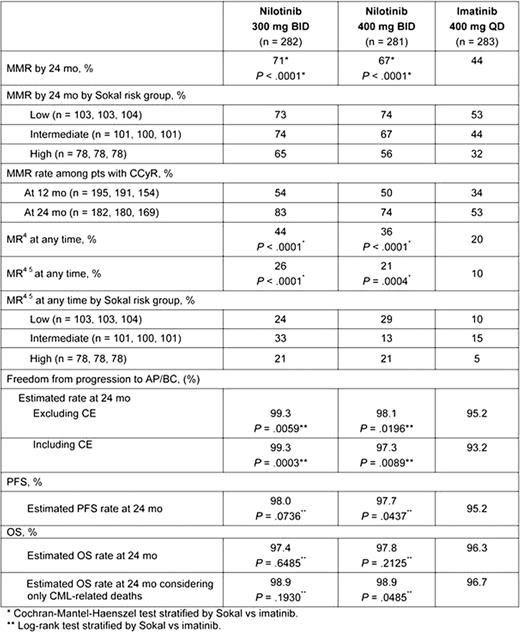
In ENESTnd, pts treated with nilotinib demonstrated higher and faster rates of major molecular response (MMR, ≤ 0.1% BCR-ABLIS), deeper molecular response (MR4, ≤ 0.01%IS and MR4.5, ≤ 0.0032%IS), and complete cytogenetic responses (CCyR) along with significantly lower rates of progression to AP/BC and fewer CML-related deaths compared with imatinib by 12 and 24 mo. Here, we report data with a minimum follow-up of 24 mo; however, efficacy and safety data based on considerably longer follow-up of ≥ 36 mo will be presented. As demonstrated in IRIS and other imatinib trials, most pts who progress on imatinib do so within the first 3 years of therapy. Thus, this 36-mo update of ENESTnd will be important to further verify the benefits of nilotinib in newly-diagnosed pts. Methods: 846 adult pts with newly-diagnosed Ph+ CML-CP were randomized to nilotinib 300 mg twice daily (BID) (n = 282), nilotinib 400 mg BID (n = 281), or imatinib 400 mg once daily (QD) (n = 283). MMR, MR4, MR4.5, time to progression to AP/BC on treatment, progression-free survival (PFS) on treatment, and overall survival (OS) were evaluated. Results: By 24 mo, both doses of nilotinib demonstrated significantly higher rates of MMR, MR4, and MR4.5 vs imatinib (Table). Nilotinib-treated pts achieved median BCR-ABLIS levels of 0.09% (300 mg BID) and 0.10% (400 mg BID) by 12 mo, while this level of reduction was not observed before 24 mo on imatinib. More pts with CCyR achieved MMR at 12 and 24 mo with either dose of nilotinib vs imatinib (Table). Regardless of Sokal risk, rates of MMR and MR4.5 were higher for nilotinib at both doses vs imatinib (Table). Progression to AP/BC (excluding clonal evolution [CE]) on treatment was significantly lower for nilotinib vs imatinib (2 pts and 3 pts with nilotinib 300 mg BID [P = .0059] and 400 mg BID [P =.0196]), respectively vs 12 pts with imatinib). After achieving CCyR, 4 pts treated with imatinib progressed to AP/BC and 2 pts treated with nilotinib 400 mg BID progressed after achieving both CCyR and MMR (1 also achieved MR4). No pt who achieved MR4.5 progressed at any time. All but 1 pt who progressed to AP/BC on treatment were in the intermediate and high Sokal risk groups; 1 pt treated with nilotinib 400 mg BID progressed in the low Sokal risk group who had an E255V mutation at progression. When considering progression events of pts after discontinuation of treatment, an additional 7, 2, and 6 events (excluding CE) were observed with nilotinib 300 mg BID, nilotinib 400 mg BID and imatinib, respectively. Twice as many pts had emergent mutations on imatinib (n = 20) vs nilotinib (n = 10 on 300 mg BID; n = 8 on 400 mg BID). At 24 mo, OS remained similar in all groups, but there were fewer CML-related deaths in both nilotinib 300 mg BID (5 pts) and nilotinib 400 mg BID (3 pts) arms vs imatinib (10 pts). Both drugs were well tolerated and few new adverse events (AEs) and lab abnormalities were observed between 12- and 24-mo of follow-up. Nilotinib 300 mg BID had the fewest discontinuations due to AEs/lab abnormalities (9% vs 13% and 10% with nilotinib 400 mg BID and imatinib, respectively). Conclusions: With a minimum follow-up of 24 mo, nilotinib continued to demonstrate superiority vs imatinib with faster and deeper molecular responses and a significantly decreased risk of progression. These data support the use of nilotinib as a standard of care option in newly-diagnosed adult pts with Ph+ CML-CP.
Saglio:Novartis Pharmaceutical: Consultancy, Speakers Bureau; Bristol-Myers Squibb: Consultancy, Speakers Bureau; Pfizer: Consultancy. Off Label Use: Nilotinib is a safe and effective treatment for patients with CML. LeCoutre:Novartis: Honoraria, Research Funding, Speakers Bureau; Bristol Myers Squibb: Honoraria. Pasquini:Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Bristol Myers Squibb: Speakers Bureau. Nakamae:Novartis: Consultancy, Research Funding, Speakers Bureau; BMS: Consultancy, Research Funding, Speakers Bureau. Flinn:nOVARTIS: Research Funding. Hochhaus:Novartis Pharmaceutical: Consultancy, Honoraria, Research Funding; Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Ariad: Consultancy, Honoraria, Research Funding; Merck: Consultancy, Honoraria, Research Funding. Hughes:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Ariad: Honoraria, Membership on an entity's Board of Directors or advisory committees. Larson:Novartis Pharmaceuticals: Consultancy, Honoraria, Research Funding. Hoenekopp:Novartis Pharmaceutical: Employment, Equity Ownership. Gallagher:Novartis: Employment. Yu:Novartis: Employment, Equity Ownership. Blakesley:Novartis Pharmaceutical: Employment. Kim:BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding. Kantarjian:Novartis: Consultancy; Novartis: Research Funding; Pfizer: Research Funding; BMS: Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal