

Abstract
Post thrombotic syndrome (PTS) is a complication of deep venous thrombosis (DVT) and is characterized by symptoms including pain, itching, heaviness, cramping, and tingling in the affected limb, which may be aggravated by physical activity. The reported prevalence of PTS in children who have had DVT varies widely from 0-70%. One of the explanations for this variability is that there has been no uniform definition or instrument used to assess PTS across studies. Since PTS is one of the most important outcome measurements in children treated for DVT, it is critical that assessment of PTS be standardized so that it is possible to compare one therapeutic approach to another. However, there are several available instruments, and no accepted “gold-standard” for comparison.
To compare the prevalence of PTS as determined by three distinct and commonly accepted PTS measurement scales. We evaluated the Villalta scale, which is a validated instrument for assessing PTS in adult patient, and compared this to two pediatric scales: a pediatric modification of the Villalata scale and the validated Manco-Johnson instrument.
We prospectively administered three different PTS outcome measurements in patients over the age of 8 years who had a history of radiologically confirmed upper or lower extremity DVT at least two months prior to participation. We chose not to evaluate younger patients since one of the objectives was to compare the adult Villalta scale to the scales developed in pediatrics. The instruments were administered sequentially by study personnel who were trained in using each instrument and blinded to the radiologic studies. A computer randomly chose the order in which they were administered.
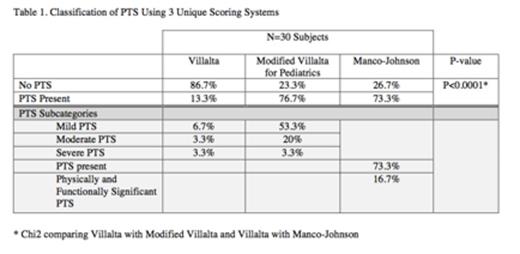
30 subjects (15 females) were enrolled in this study with a mean age of 16.8 yrs (S.D. 4.1 yrs). All but four patients were over the age of 14 years at the time of assessment. The majority of subjects 25/30 had a lower extremity DVT, while 5 had an upper extremity DVT. The average duration since DVT to PTS determination was 3.9 yrs (S.D 3.9 yrs). The proportion of subjects classified as having PTS using the Villalta scale was 13%, which was significant less than either of the other scales in which 73% (Manco-Johnson) and 76% (Modified Villalta) of patients were classified as having PTS, p< 0.00001 (Table 1). The majority of patients with PTS as determined by the modified Villalta scale had mild PTS (16/23). Similarly, the majority of patients with PTS as determined by the Manco-Johnson instrument did not have functionally significant PTS (17/22).
There was significant discordance in the Villalta scale compared to the two pediatric scales, despite the fact that the majority of the patients were teenagers. This is especially relevant when considering the best measurement to be used in long-term follow-up of these patients, particularly for comparing outcomes of interventional therapies, such as thrombolysis. The primary difference between these instruments is that subjects needed to have a score of ≥5 to be classified as having PTS using the Villalta score (requiring more than one sign or symptom) compared to a score of ≥1 (any abnormal sign or symptom) on the modified and Manco-Johnson scale. This study demonstrates that the presence of PTS, as defined by these scales, is not a well-defined or standardized outcome, particularly when comparing adult and pediatric instruments.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal