

Abstract
Approximately 30% of diffuse large B-cell lymphoma (DLBCL) patients relapse following initial immuno-chemotherapy. DLBCL usually arises without a history of lymphoma (“de novo”), but can also transform from antecedent indolent lymphoma. There are limited data regarding the outcomes of the two subpopulations of transformed and de novo DLBCL patients treated with second-line chemotherapy regimens. We sought to compare the outcomes of relapsed/refractory transformed and de novoDLBCL patients after receiving frontline rituximab, cyclophosphamide, doxorubcin, vincristine and prednisone (R-CHOP) and second-line rituximab, ifosfamide, carboplatin and etoposide (R-ICE) chemotherapy prior to planned autologous stem cell transplant (ASCT). This analysis was performed on an intent-to-treat basis.
This retrospective review compared 100 consecutive DLBCL patients, 89 de novo and 11 transformed, at the Cleveland Clinic between 2000 and 2012. Inclusion criteria were: age ≥18 with relapsed/refractory DLBCL, prior treatment with R-CHOP and second-line R-ICE chemotherapy. Baseline characteristics were compared for categorical variables using the Chi-square test or Fisher's exact test; continuous and ordinal categorical variables were compared using the Wilcoxon rank sum test. Overall survival (OS) and progression-free survival (PFS) in transformed and de novorelapsed/refractory DLBCL patients were estimated using the Kaplan-Meier method and compared using the log-rank test. Stepwise multivariable analysis with a variable entry criterion of P<0.10 and a variable retention criterion of P<0.05 was used to identify multivariable prognostic factors.
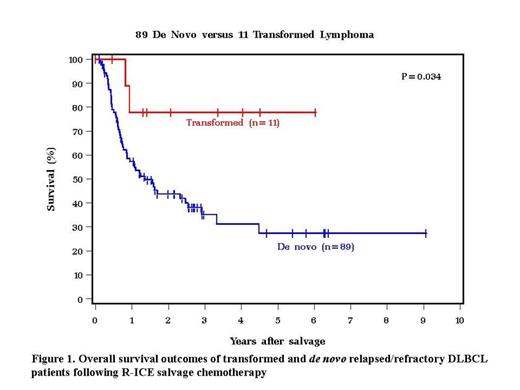
The majority of patients had advanced stage (III or IV) disease at the time of diagnosis of DLBCL (62.5% for transformed and 68.5% de novo patients, P = 0.59).There was a male predominance in both groups, transformed (72.7%) and de novo (61.8%), P = 0.48. The median age at second-line was comparable between transformed and de novo patients (62 vs. 58 yrs, respectively, P = 0.66). The period of time between R-CHOP and R-ICE was significantly longer in transformed patients than those with de novo DLBCL (30.1 vs. 11.3 months respectively, P< 0.001). The number of cycles of R-ICE was comparable between the two groups and most commonly was 3. The percentage of patients who proceeded to a planned ASCT was comparable for transformed and de novo patients (45.5% vs. 47.2% respectively; P = 0.97). The molecular subtype for cases in which data were available was germinal center in 6 of 7 (85.7%) transformed patients and 32 of the 46 (69.6%) de novo cases as determined by the Hans immunohistochemistry algorithm (P = 0.66). Transformed patients had a statistically significant improvement in OS compared with de novo patients (77.8% vs. 27.4% 5 year OS, respectively, p=0.034). Death due to relapsed disease was comparable for both transformed and de novo patients (50% vs. 38.5% respectively). Transformed patients had marginally better PFS outcomes after 5 years (51.4%) than de novopatients (26.9%; p=0.18). In a multivariable analysis, transformed DLBCL was associated with a statistically significant odds ratio (OR) of 0.23 (95% confidence interval (C.I.) 0.05 – 0.95)1.05 -17.8) for OS (p=0.043). ASCT was associated with improved OS in multivariable analysis (OR = 0.57 (C.I. 0.33 – 1.00), p= 0.05).
Contrary to expectation, transformed DLBCL patients previously treated with R-CHOP have superior OS after second-line R-ICE than patients with de novo DLBCL. This may result from relatively longer period of time between initial treatment and the need for second-line and possibly an enrichment for cases with the more favorable germinal center molecular subtype. Improvements in second-line treatment for de novo relapsed/refractory DLBCL with novel agents are needed.
Hill:Celgene: Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal