

Abstract

Eltrombopag, a thrombopoietin receptor agonist (TPO-RA), increases platelet counts in patients with cITP. TPO-RAs have been associated with varying degrees of bone marrow (BM) reticulin increases. Patients in the EXTEND study, an ongoing, open-label extension study of eltrombopag in patients with heavily pretreated cITP who received eltrombopag or placebo in a previous eltrombopag study, underwent annual BM biopsies while on study.
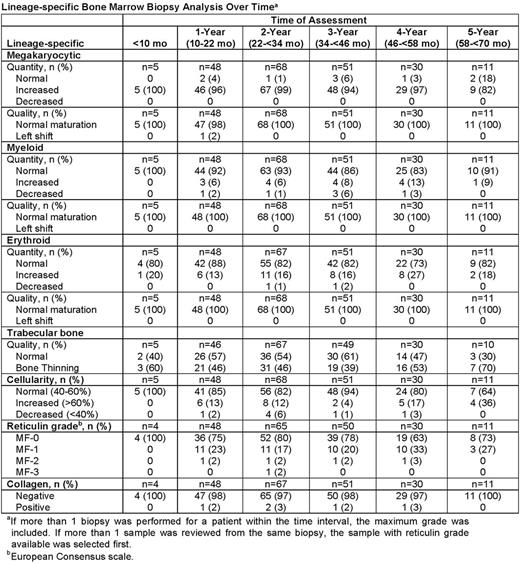
Central morphology review was done by 2 hematopathologists blinded to clinical information who assessed specimens for cellularity, megakaryocyte, erythroid, and myeloid quantity and appearance; trabecular bone changes; and reticulin and collagen deposition (European Consensus scale).
In EXTEND, 302 patients with cITP were treated with eltrombopag for ≤6.5 years as of February 2013. Of these, 232 BM biopsy specimens collected from 117 patients from pretreatment and up to 5.5 y on treatment were available at the time of this analysis, and were centrally reviewed (Table). Of these, 5 patients provided a biopsy sample within <10 mo on treatment, 48 patients at 1 y, 68 at 2 y, 51 at 3 y, 30 at 4 y, and 11 at 5 y on treatment.
Median age (range) of the 117 patients was 50 (20-78) y; 69 (59%) patients were female; 85% were Caucasian/European, 9% were East Asian, 2% were South East Asian, and 4% were Arabic/North African. Median time since ITP diagnosis was 58.6 (8.5-421) mo.
Two hundred and nine on-treatment biopsies, collected from 115 patients, were graded for reticulin using the European Consensus scale. Most (63-80%) of the on-treatment biopsies, collected between 1 y and 5 y, were MF-0 or MF-1 (17-33%) (Figure). Reticulin fibers were increased (MF ≥2) in 5 specimens from 2/115 (1.7%) patients. All 5 specimens were positive for collagen, and 3 of the 5 specimens in the 2 patients were judged as hypercellular. Of the 2 patients, 1 patient (East Asian) had reticulin documented after 2 y (970 days) of treatment, and was preemptively withdrawn from the study. Per protocol, a post-treatment biopsy was performed; a BM specimen taken 7 mo following withdrawal was graded as MF-0 for reticulin and negative for collagen. The second patient (Caucasian) had MF-2 at 1 y, which increased to MF-3 at 2 y and contained megakaryocytes with myeloproliferative neoplasm-like features, and then returned to MF-2 at the 3 y and 4 y assessments; however, these biopsies at 3 y and 4 y showed no signs of myeloproliferative neoplasm-like features and had reverted to normal. The patient remains on treatment at the time of this analysis. Neither patient experienced any adverse event or abnormality in hematologic parameters potentially related to impaired BM function.
Cellularity was normal in the majority of patients at each assessment timepoint. Most (82-99%) patients demonstrated megakaryocytic hyperplasia. Megakaryocyte morphology was normal in all patients in all years except for 1 patient in year 1. Seven patients (6%) had megakaryocytes reminiscent of those seen with polycythemia vera or essential thrombocythemia. Erythroid hyperplasia was observed in 13-27% and myeloid hyperplasia in 6-13% of patients. Trabecular bone thinning was found in 39-70% of patients over the 5-year observation period. No pathologic pattern of changes was identified among the on-treatment specimens.
Reticulin fibrosis was considered a potential risk for cITP patients receiving TPO-RAs. In the ongoing EXTEND study, at the time of this analysis, reticulin was either absent or mildly increased in 113/115 (98%) patients treated with eltrombopag up to 5.5 years at the time of their biopsy. No patient with reticulin or collagen increases showed clinical signs or symptoms indicative of BM dysfunction, and the findings were reversible upon discontinuation of treatment. No pattern of increasing reticulin deposition with longer treatment periods was observed based on BM biopsy data available to date. These data suggest that for most cITP patients, treatment with eltrombopag is not associated with the development of BM reticulin or collagen fibrosis; however, the potential association of TPO-RAs and increased BM fibrosis in cITP still needs to be better understood.

Brynes:GlaxoSmithKline: Research Funding. Bakshi:GlaxoSmithKline: Employment, Equity Ownership. Bailey:GlaxoSmithKline: Employment, Equity Ownership. Chan:GlaxoSmithKline: Employment.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal