

Abstract
We have previously defined poor graft function (PGF) as 2 or 3 cytopenic lines (Hb<10 g/dl, neutrophil count <1,0 x 10^9/L, platelet count <30 x 10^9/L), lasting for at least 2 consecutive weeks post-transplant, beyond day +14, with transfusion requirement, associated with hypoplastic-aplastic bone marrow, in the presence of complete donor chimerism and in the absence of severe GVHD and relapse (Larocca 2006). We have also shown that PGF can be treated with the infusion of donor CD34+ cells, selected from mobilized peripheral blood. (Larocca 2006) .
To update the 2006 study in 41 patients.
All 43 patients received a boost of CD34+ selected peripheral blood stem cells (PBSC) without prior conditioning and without GvHD prophylaxis. The median age of patients was 37 years (18-60y). The median number of CD34+ PBSC infused was 3.45 x106/Kg at median days of 140 days from 1st HSCT.
Complete response, or tri-lineage recovery was defined as achieving Hb >10 g/dl, ANC > 1000 x109/L, platelets > 100.000 x 109/L. A partial recovery was defined as transfusion independence, without a complete hematologic recovery. The median follow up was 1245 days.
Tri-lineage recovery was seen in 31/41 (76%) and 3/43 patients became transfusion independent, for an overall response of 83%). The median time for complete hematological recovery from CD34+ boost infusion was 183 days.
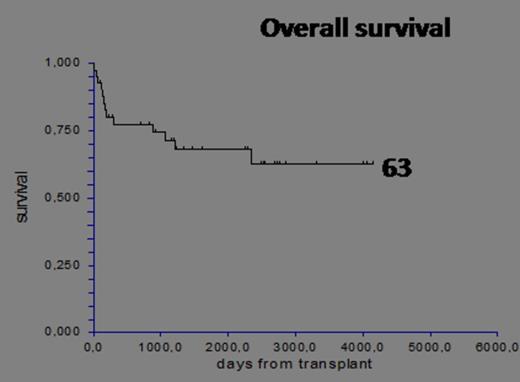
There was no influence on tri-lineage recovery of the following factors : dose of CD34 cells (</> 3.3) (78% vs 72%), nor patient age (</>35 years) 75% vs 76%, nor donor type (HLA id sib 83%, UD 79%, family mm 68%). All the patients who achieved tri-lineage recovery are alive and disease free (28/41 patients). In this cohort 13 patients died due to relapse 9/14 (64%) or GVHD 2/14 (14%) or other causes 2/14 (14%). The overall actuarial survival is 63% with a median follow up of 1245 days (94-4151 days).
We confirm that infusion of CD34+ selected PBSC is associated with a high rates of tri-lineage recovery, with low risk of acute or chronic GVHD in patients who develop poor graft function following an HSCT. Tri-lineage recovery or achieving transfusion independency have an interesting impact either on disease free and overall survival.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal