

Abstract
Background: Paroxysmal nocturnal hemoglobinuria (PNH) is an acquired clonal bone marrow disorder caused by a somatic mutation in PIGA that leads to a marked deficiency or absence of the complement regulatory proteins CD55 and CD59. The disease manifests with intravascular hemolysis, anemia and thrombosis. PNH is characterized by diverse changes in iron metabolism. Chronic hemolysis leads to the massive iron loss due to hemoglobinuria and hemosiderinuria, whereas frequent transfusions in severely anemic, transfusion-dependent patients might cause the development of iron overload.
Aim: to assess iron metabolism in PNH patients based on both laboratory parameters and MRI data.
Methods: the study group included 28 PNH patients (pts) followed up in our Center between 2015 and 2017. Laboratory parameters including hemoglobin (Hb), reticulocytes (RET), erythrocyte and granulocyte PNH clone sizes and LDH levels were analyzed. Iron metabolism was characterized by measurement of serum ferritin (SF), transferrin, iron concentration, total iron binding capacity (TIBC), transferrin saturation (TS). Multiecho gradient-echo T2* magnetic resonance imaging (T2* MRI) was performed to assess both liver and kidney iron load. All pts were divided into 3 cohorts: №1 - pts on treatment with eculizumab, №2 - pts who received eculizumab in the past and №3 - eculizumab naïve pts.
Results:Сohort №1 included 2 pts (2 women) aged 39 and 64 yrs. Hb level was 9,3 and 9,9 g/dl, RET count - 9,6 and 10%, LDH level - 570 and 650 U/l. Erythrocyte PNH clone size was 99 and 72%, and granulocyte PNH clone size was 99 and 87%.
Cohort №2 consisted of 6 pts (2 men and 4 women, median age 39 yrs (31 - 53)) which had a history of eculizumab treatment. The median duration of eculizumab treatment in these pts was 23 months, the median time of treatment cessation (due to administrative reasons) was 6 months before study assessments. The medians of laboratory parameters were as follows: Hb = 7,7 g/dl, RET count = 6,6%, LDH level = 3296 U/l (1580 - 7444), erythrocyte PNH clone size = 36%, granulocyte PNH clone size = 98%.
Cohort №3 consisted of 20 untreated pts (15 men and 5 women, median age 35 yrs (29 - 58)). The medians of laboratory parameters: Hb = 8,4 g/dl, RET count = 8,5%, LDH level = 4130 U/l (670 - 8322), erythrocyte PNH clone size = 52%, granulocyte PNH clone size = 93%.
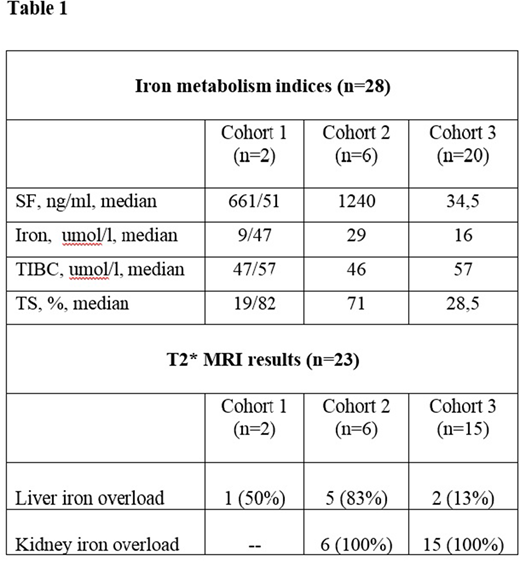
Serum iron metabolism indices in all patient cohorts are reported in Table 1. Based on the analysis of the measured serum iron metabolism indices, 3 types of iron metabolism disturbances were identified in pts of the study group (n=28): iron deficiency (14% of pts), iron overload (21% of pts) and divergent changes (65% of pts). T2* MRI was performed in 23 pts. Signs of liver iron overload were revealed in 35% pts whereas signs of kidney iron overload were detected in 91% pts. T2* MRI data was analyzed within each of the patient cohorts, results are reported in Table 1.
Conclusion: the results of our pilot study demonstrate that in PNH patients laboratory parameters are not sufficient to assess iron metabolism. T2* MRI is a noninvasive and accurate technique which should be considered as a method of choice to quantify tissue iron overload. Kidney iron overload was detected in all PNH patients who did not receive eculizumab at the moment of the analysis and was absent in 2 patients on eculizumab. Thus, hemosiderin deposition in the renal cortex might play an important role in the development of renal involvement including the formation of interstitial fibrosis and chronic kidney disease.
Lukina:Sanofi Genzyme: Honoraria, Other: Principal investigator in the eliglustat Phase 2, ENGAGE, ENCORE, and EDGE trials; receives travel reimbursement; member of advisory boards, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal