

Abstract
The clinical significance of 18F-fluorodeoxyglucose(FDG) positron emission tomography/computed tomography (PET/CT) in the diagnostic approach of multiple myeloma (MM) remains incompletely elicited. Little is known about the value of bone marrow (BM) imaging pattern assessed by PET/CT in MM. And no standardized imaging interpretation criteria have been established to define different imaging pattern. Besides, the lack of standardized interpretation criteria hampered the routine use of PET/CT and led to low interobserver reproducibility in interpreting results. We herein report a study that aimed at finding out the appropriate interpretation criteria to define different tracer uptake pattern on PET/CT and analyzing the prognostic implications of baseline BM FDG uptake pattern in patients with multiple myeloma.
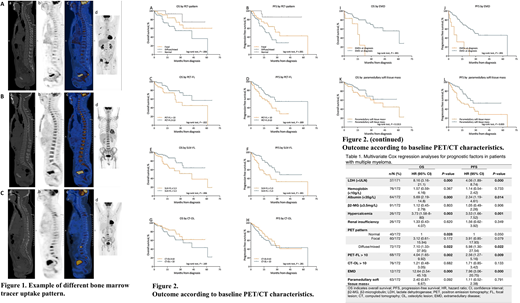
We retrospectively studied 52 healthy individuals who had undergone PET/CT scan for cancer screening and 172 newly diagnosed MM patients. In our healthy cohort, BM FDG uptake (represented by the average SUVmean of L1 and L2 vertebral body) were higher than that of liver (SUVmean), spleen (SUVmean) and mediastinal blood pool (SUVmax) in 1 (1.9%), 11 (21.2%) and 4 (7.7%) patients, respectively, in physiological status. Hence, we proposed new PET/CT interpretation criteria for evaluation of BM tracer uptake pattern in MM. According to these criteria, 60 (34.9%) patients had focal (focal lesion in BM with FDG uptake higher than liver, Figure 1A), 6 (3.5%) had diffuse (diffuse homogenous BM FDG uptake higher than liver, Figure 1B), 66 (38.4%) had mixed pattern (innumerable hypermetabolic foci on a background of BM with diffusely increased tracer uptake, Figure 1C) and 40 (23.3%) had normal BM uptake. The bone marrow FDG uptake was correlated to bone marrow plasma cell infiltration rate (r = 0.228, P < 0.01). Besides, plasma cell infiltration rate differed in different uptake pattern: patients with diffuse/mixed bone marrow FDG uptake pattern had the highest mean bone marrow plasma cell infiltration rate, followed by those with focal pattern (Kruskal-Wallis test, P < 0.0001). Furthermore, BM tracer uptake pattern demonstrated correlations with prognostically relevant baseline parameters: diffuse/mixed pattern was correlated with higher BM plasma cell infiltration rate, more advance ISS stage, lower hemoglobin level, higher level of β2-microglobulin and serum creatinine. Diffuse/mixed BM tracer uptake pattern (Figure 2A-B), more than ten FDG-avid focal lesions (PET-FL) at baseline (Figure 2C-D), presence of extramedullary disease (EMD, Figure 2I-J), and a standardized uptake value (SUV-FL) > 5.3 (Figure 2E-F) adversely affected estimated 3-year progression free survival (3-yr PFS; diffuse/mixed pattern: 26.8%; PET-FL > 10: 54.2%; EMD: 0.0%; SUV-FL > 5.3: 32.5%) and overall survival (3-yr OS; diffuse/mixed pattern: 50.6%; PET-FL > 10: 44.8%; EMD: 0.0%; SUV-FL > 5.3: 51.0%). Presence of paramedullary soft tissue lesion adjacent to bone marrow shortened PFS with borderline adverse influence on OS (Figure 2K-L). Clinical outcomes were not significantly influenced by the number of osteolytic lesion on CT images (Figure 2G-H). In multivariate analysis (Table 1), the following factors were found to be independent prognostic factors for inferior outcome: diffuse/mixed BM uptake pattern, PET-FL > 10, EMD, hypercalcemia, hypoalbuminemia and level of blood lactate dehydrogenase > upper limit. Diffuse/mixed BM FDG uptake pattern was an independent predictor associated with inferior OS (HR 7.10; 95% CI 1.33-37.95) and PFS (HR 5.98; 95% CI 1.30-27.54).
In conclusion, we propose an FDG uptake higher than that of liver is an appropriate positivity cut-off to discriminate physiological and pathological uptake in bone marrow for patients with multiple myeloma. With these interpretation criteria, the bone marrow PET/CT pattern can be defined as four types: normal, focal, diffuse and mixed. A diffuse/mixed BM FDG uptake pattern is a reliable predictor of inferior outcome.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal