

Abstract
Introduction
Bortezomib, a proteasome inhibitor and lenalidomide (Len), an immunomodulatory drug are the backbone of established treatment regimens for newly diagnosed MM. Patients with dual-refractory (refractory to both bortezomib and lenalidomide) disease have a poor prognosis with overall survival estimated to be less than one year. Pomalidomide (Pom) has distinct anticancer, antiangiogenic and immunomodulatory properties and has demonstrated synergistic antiproliferative activity in combination regimens. The aim of our study is to compare different Pom based regimens to identify the most effective regimen for relapsed refractory multiple myeloma (RRMM) patients.
Methods
A comprehensive literature search was performed on PubMed, Cochrane library, Web of Science, Embase and AdisInsight databases on 03/29/2018 which identified a total of 1374 studies. We included phase II/III clinical trials on pomalidomide based regimens that have clearly documented efficacy outcomes. All statistical analyses were performed using Comprehensive Meta-analysis (CMA) Version 3. We used the Cochrane Q statistics (p<0.05 considered significant) and I2 index to calculate the degree of heterogeneity of the studies. A random effect model was used if there was significant heterogeneity (p>0.05 or I2 >50%). Studies were classified into subgroups according to the therapeutic regimen: dual and triplet combinations. A separate stratified analysis of triplet regimens based on type of regimen was also performed.
Results
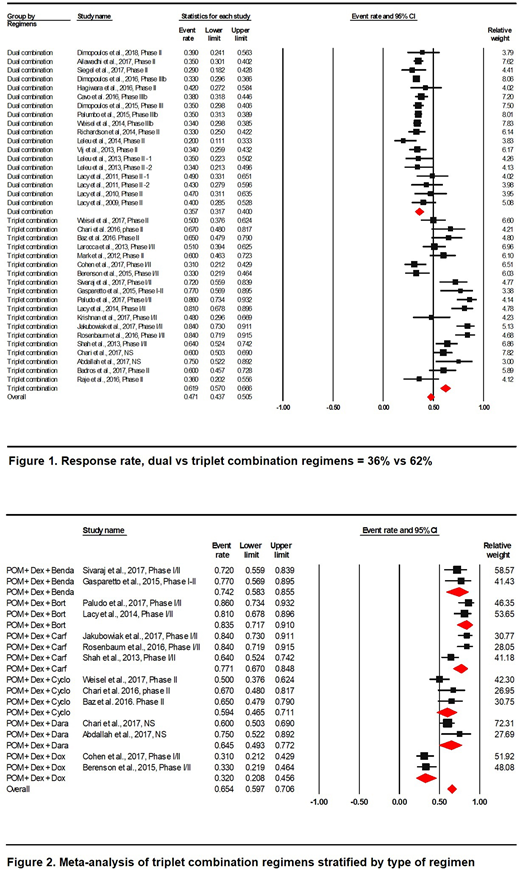
A total of 35 studies (n = 4623 patients) were included. The most commonly studied regimen was Pom + LoDex (Low dose dexamethasone) with a total of 16 studies on this regimen. All patients included in our study had ≥ 2 prior lines of therapy. Mean number of prior lines of therapy was 6. Most patients were lenalidomide refractory, with 10 patient cohorts of 100% refractoriness and 8 cohorts of ≥ 90% refractoriness. Pooled analysis showed an overall response rate (ORR) of 47.1% across all Pom regimens including both doublet and triplet regimens. An I2 value of 87.3 was found, indicating high heterogeneity across all Pom regimens. With Pom-LoDex, pooled ORR was found to be 35.7% and mean OS 14.37 months. With triplet regimens, pooled ORR was found to be 61.9%. In a separate stratified analysis of triplet regimens based on type of regimen, pooled ORRs with few selected regimens were as follows; Bort-Pom-LoDex (pooled ORR 83.5%, mean PFS 15.7 months [mos]), CFZ-Pom-LoDex (pooled ORR 77.1%, mean PFS 15.3 mos), Pom-LoDex-bendamustine (pooled ORR 74.2%), Pom-Dex-daratumumab (pooled ORR 64.5%), Pom-LoDex-cyclophosphamide (pooled ORR 59.4%, mean PFS 9.5 mos), Pom-LoDex-doxorubicin (pooled ORR 32%).
Most frequently reported adverse event with Pom based regimens was myelosuppression. Mean incidences of grade ≥3 hematologic adverse events were neutropenia (47.6%), anemia (26.5%), and thrombocytopenia (20.8%). Mean incidences of grade ≥3 non-hematologic adverse events were infections (29.1%), pneumonia (13.8%) and fatigue (10%). Most of the studies used pomalidomide 4mg daily dosing. Lacy et al. suggested no advantage of 4mg pomalidomide over 2 mg daily dosing.
Conclusion
From results of pooled analysis, we can infer that triplet combinations of Pom yield almost double response rates (pooled ORR 61.9%) when compared to dual combination of Pom-LoDex (pooled ORR 35.7%). Among three drug combinations, Bort-Pom-LoDex (pooled ORR 83.5%) and CFZ-Pom-LoDex (pooled ORR 77.1%) seem to produce better outcomes. Our study provides useful insight into relative efficacy of various Pom regimens for treatment of RRMM patients. Several trials involving various MoAbs like nivolumab, daratumumab, elotuzumab, isatuximab and pembrolizumab in combination with Pom-LoDex are currently ongoing. Pomalidomide has an acceptable safety profile. Most common treatment emergent adverse events were myelotoxicity and infections that can be effectively managed with supportive care and dose modifications.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal