

Abstract

Background: Anticomplement C5 therapy with eculizumab is the standard of treatment of patients (pts) with active hemolytic PNH. However, there are few data on long-term complement inhibition efficacy and current PNH prognosis from real-world clinical practice.
Objectives: The aim of this study was to evaluate long-term eculizumab efficacy and PNH outcomes in the large cohort in Russia.
Methods: As of August 1, 2018, a total of 354 pts with hemolytic PNH were observed in the I.P. Pavlov First St. Petersburg State Medical University in cooperation with the local hematological service in 75 regions of Russia (n=344), as well as in Belarus, Kazakhstan, Kyrgyzstan, Ukraine, Tajikistan (n=10) (Table 1). The analysis was conducted in the whole cohort and separately in the prospective phase after November 2011 with the eculizumab availability in Russia.
We analyzed indications and access to anticomplement C5 therapy according to National guidelines (2014), frequency and causes of discontinuation of therapy, cumulative incidence of independence from transfusions with allo-HSCT as competing risk, frequency of breakthrough hemolysis (BTH) and intensive extravascular hemolysis, overall survival (OS) and causes of mortality.
Results: According to the current National guidelines (2014), 323 pts had at least one indication for therapy with eculizumab: thrombosis (n=89, 25 %), transfusion-dependent hemolytic anemia (n=261, 74 %), acute kidney injury (AKI, n=69, 19 %), chronic kidney disease (CKD, n=244/304, 80 %) including CKD stage ≥ 2 (n=66/304, 22 %), pulmonary hypertension (n=66/265, 25 %) and pregnancy (n=22). Due to differences in regional support for rare diseases, only 204 (63%) pts had access to therapy with eculizumab. In addition, 19 pts received novel anti-C5 agent in clinical trial and were excluded from analysis. Allogeneic HSCT was performed in 24 pts, including 2 cases of MDS/AML evolved from AA/PNH and 17 cases of severe AA/PNH with eculizumab bridging in the prospective phase.
With the median duration of eculizumab therapy of 3.4 years (0.2-6.1) the independence from RBC transfusions (TI) was achieved in 109 of 154 initially transfused pts (71 %) with a cumulative incidence of 61 % (95 % CI, 52-68) and 69 % (95 % CI, 60-76) after 12 and 24 months of therapy respectively. The median hemoglobin level at last follow-up were 6.6 (4.0-9.7), 10.5 (range, 7.1-15.4) and 12.1 g/dl (8.9-14.0) in patients who did not reach the TI, who reached the TI and were never transfused, respectively (p =0.0001).
BTH was documented in 36 of 184 evaluated pts (20 %), including 16 and 20 cases with and without obvious triggers respectively. Intensive extravascular hemolysis with bilirubin level > 2xULN persisted in 31 % pts. Temporary or permanent discontinuation of eculizumab treatment occurred in 58 pts due to death (n=11), allogeneic BMT (n=17), spontaneous clone reduction (n = 4), absence of new indications 6 months after delivery (n=4), and terminating access to treatment (n=22). All pts of the latter group developed a relapse of intensive intravascular hemolysis, which in 3 cases was complicated by AKI (n=1), stroke (n=1) and myocardial infarction (n=1).
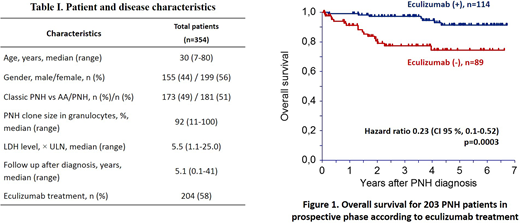
OS was assessed in the prospective phase after 2011. A total of 24/203 (12 %) pts died which resulted in 5-year OS of 87% (CI 95 %, 81-92). Treatment with eculizumab significantly improved OS (Fig.1). The 5-year OS rate was 91% (CI 95 %, 85-98) in pts treated with eculizumab and 74 % (CI 95 %, 63-85) in never-treated pts (p=0.0003). There were significant differences in the causes of death between pts receiving and not receiving eculizumab: related to thrombosis 1/7 (14 %) vs 9/17 (53 %), AA and MDS 4/7 (57%) vs 5/17 (29 %).
Conclusions: The results of the study show both the high efficacy and limitations of treatment with eculizumab for PNH in real-world practice. Prospectively confirmed significant improvement of the overall survival on eculizumab stress the need for faster and wider access to costly therapy. Nevertherless, a number of limitations, including BTH and extravascular hemolysis, lack of control of bone marrow failure and further clonal evolution, determine the relevance of next-generation complement inhibitors and risk-adjusted allogeneic HSCT as a curative option.
Kulagin:Alexion Pharmaceuticals, Inc: Consultancy, Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal