

Abstract
Introduction: Contemporary data describing treatment patterns, adverse events (AEs) and outcomes in CLL patients in clinical practice is lacking. We conducted a retrospective cohort study and assessed treatment patterns, AEs, health care resource use (HCRU), and costs in patients with newly diagnosed CLL.
Methods: Using a nationally representative population of privately insured patients in the US, adult patients with CLL were selected if they had continuous health plan enrollment for ≥12 months before the first CLL diagnosis without any evidence of any CLL-directed treatment. Treatment patterns up to 4 lines of therapy (LOT) and occurrence of AEs during CLL therapies were assessed. Mean per-patient monthly HCRU and costs were assessed overall and by number of unique AEs.
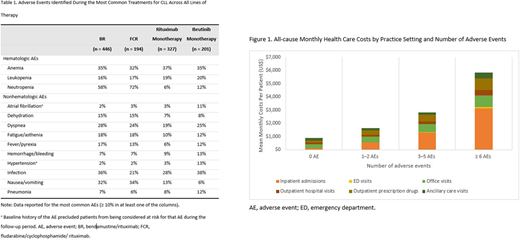
Results: Of all patients meeting the selection criteria (n=7,639; median age, 66 years), 18% (n=1,379) received a systemic therapy during study follow-up. The most common systemic therapy regimens, regardless of therapy line, were bendamustine/rituximab (BR) (32%), rituximab monotherapy (24% [including maintenance]), ibrutinib monotherapy (15%), and fludarabine/cyclophosphamide/ rituximab (FCR) (14%). Of these, BR was the most common LOT-1 regimen (28.1%), while ibrutinib was the most common regimen in LOT-2 (20.8%) and in LOT-3 (25.5%). Use of idelalisib was limited to 1.6% of all patients receiving systemic therapy; however, an increasing trend was observed as patients moved from first to fourth LOT (<1% in LOT-1, 3.1% in LOT-2, 4.7% in LOT-3, and 8.6% in LOT-4). AEs identified during the most common treatments for CLL are presented by treatment regimen in Table 1. The mean monthly all-cause and CLL-related costs, among patients treated with a systemic therapy, were $7,943 (SD=$15,757) and $5,185 (SD=$9,935), respectively. Figure 1 depicts mean monthly costs by care setting and number of AEs, among all patients. Mean (SD) monthly all-cause costs during the post-index date follow-up were $905 ($1,865) among those with no AEs, $1,655 ($5,364) among those with 1-2 AEs, $2,883 ($8,483) among those with 3-5 AEs, and $6,032 ($13,290) among those with ≥6 AEs.
Conclusions: This population-based study yielded recent real-world evidence on treatment patterns, AEs, HCRU, and costs in patients enrolled in health plans in the US. Immunochemotherapy, particularly BR, remained the preferred frontline therapy for CLL, whereas ibrutinib was the preferred therapy in LOT-2 and LOT-3, during the study period. This study demonstrates that the AE burden associated with current treatment alternatives for CLL is substantial, and the management of AEs occurring during treatments may have a significant impact on the overall health care costs.
Kabadi:AstraZeneca: Employment. Goyal:RTI Health Solutions: Employment, Research Funding. Nagar:RTI Health Solutions: Employment, Research Funding. Kaye:RTI Health Solutions: Employment, Research Funding. Davis:RTI Health Solutions: Employment, Research Funding. Mato:Celgene: Consultancy; AstraZeneca: Consultancy; Pharmacyclics: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy; Sunesis: Honoraria, Research Funding; TG Therapeutics: Research Funding; Janssen: Consultancy, Honoraria; Acerta: Research Funding; Prime Oncology: Speakers Bureau; Regeneron: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal