

Abstract
Background: Over-expression of Aurora A has been shown in many subtypes of non-Hodgkin lymphoma (NHL) and is a negative prognostic factor in mantle cell lymphoma (MCL), where expression correlates with tumor proliferative signature (Ki67), and may contribute to cell cycle dysregulation. Aurora A regulates chromosomal stability through effects on mitosis and cell cycle regulation. Bortezomib increases both pro-apoptotic proteins and cell cycle dependent kinase inhibitors. Thus, there is a strong scientific rationale to combine Aurora A kinase and proteasome inhibition. We evaluated the combination of alistertib, an oral Aurora A kinase inhibitor, with bortezomib and rituximab in a CTEP sponsored phase 1 study of patients with relapsed /refractory (RR) low grade NHL or MCL.
Methods: Patients with RR low grade NHL or MCL, who had received at least one line of immuno-chemotherapy were treated according to a 3 + 3 design with 3 dose escalation cohorts (DL1, DL2, and DL3) to identify the recommended phase 2 dose (RP2D) with an expansion cohort at the RPTD. Patients received alisertib 30mg BID (DL1 and DL2) or 40mg BID (DL3) on days 1-7, bortezomib subcutaneous 1mg/m2 (DL1) or 1.3 mg/m2 (DL2 and DL3) on days 1, 8, and 15, and rituximab 375mg/m2 on day 1 for the first 8 cycles, and subsequently q 3 months. An expansion cohort was treated at DL3. Treatment cycles were 28 days. Dose Limiting Toxicity (DLT) was defined within the first cycle of therapy.
Results: A total of 24 patients at 3 sites were enrolled between 06/2013 and 02/2018, including DL1: 3, DL2: 7; DL3: 14. Median age was 64 (range 46-87). Twelve patients (50%) were male. Nineteen patients had low grade NHL, and 5 patients had MCL. Performance status was 0-1 in 22 (92%) patients, and 2 in 2 (8%) patients.
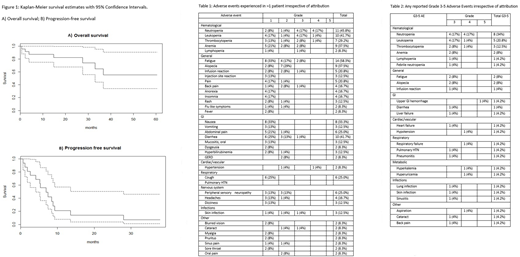
Dose Escalation and Safety: The recommended phase II dose (RP2D) was DL3, with the only DLT in DL3 (prolonged grade 4 neutropenia). The most common grade 3-4 AEs at all dose levels were neutropenia (34%), thrombocytopenia (13%), anemia (8%), and fatigue (8%); grade 2 alopecia occurred in 37% (Table 1). Other grade 4 AEs included hypertension & hypotension, respiratory failure, hyperkalemia and hyperuricemia (n=1 (4%) each); one patient died of GI hemorrhage deemed unrelated to study treatment (NSAID overdose). Grade 3 neutropenia and leukopenia was seen in 4 patients and thrombocytopenia in 1. There was one grade 3 AE each of: hypertension, pulmonary hypertension, pneumonitis, fatigue, diarrhea, infusion reaction, lung infection, and febrile neutropenia.
Efficacy: A total of 18 patients were evaluable for response. Five patients were not evaluable for response for the following reasons: withdrawal of consent (3, 1 each DL1, 2, 3), non-compliance (1 DL2), and death unrelated to study drug (1, DL2). For patients who were treated with at least 3 cycles of therapy, and had a restaging CT scan, the median duration of therapy was 142 days, (range 29-590). Response was seen in 7/18 evaluable patients for an overall response rate (ORR) of 38%; 4 of 18 patients (22%) had a complete response (CR), and 4 of 18 patients (22%) had a partial response (PR). An additional 8/18 patients (44%) had stable disease for a clinical benefit rate of 88%. With a median follow-up of 30.9 months, the median PFS was 6.9 months (95%CI 4.1-28.0) and median OS not reached. OS at 3 years was 64.9% (95% CI 44.1-95.3%; Fig. 1). Median duration of response was 14.1 mo (95% CI 2.63-NR).
Conclusion: Alisertib in combination with bortezomib and rituximab is a well-tolerated regimen with significant and durable activity in heavily pretreated low grade NHL and MCL. The RP2D is DL3 (R + bortezomib 1.3mg/m2 and 1.8 alisertib 40mg bid). A correlation of Aurora Kinase tumor expression with clinical outcome is planned.
Barta:Janssen: Membership on an entity's Board of Directors or advisory committees; Merck, Takeda, Celgene, Seattle Genetics, Bayer: Research Funding. Diefenbach:Merck: Consultancy, Research Funding; Genentech: Consultancy; Incyte: Research Funding; Millenium/Takeda: Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Acerta: Research Funding; Seattle Genetics: Consultancy, Research Funding; Trillium: Research Funding; Denovo: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal