

Abstract
Background: Prior to the approvals of ibrutinib (ibr), idelalisib, and venetoclax, data from the Connect CLL registry showed that across 199 US centers only 65% of patients (pts) had FISH testing and 6% had IGHV testing performed prior to the first chronic lymphocytic leukemia (CLL)-directed treatment (tx), and 40% had repeat FISH testing prior to a subsequent therapy (Mato, Br J Haematol 2016). In today's era, molecular-genetic testing should be universally performed to guide tx decisions for pts with CLL, particularly for pts with 17p deletion (del[17p]), TP53 mutation, and/or unmutated IGHV (U-CLL), as recommended by several guidelines. Whether the widespread availability of novel agents has improved prognostic testing patterns and if those results are appropriately utilized in selecting therapies remain important unanswered questions. InformCLL (NCT02582879) is a US, multicenter, prospective, observational real-world registry of pts with CLL receiving various lines of tx across 150 centers (96% community, 4% academic). This analysis describes rates of prognostic testing in pts with CLL stratified by line of therapy, proportions of pts with specific abnormalities, and current tx patterns in clinical practice in this registry.
Methods: Enrollment began in Oct 2015. Eligible pts had to be ≥18 years (y), start approved anti-CLL tx within 30 days of enrollment, and provide consent. First tx at enrollment was classified into 5 groups: chemoimmunotherapy (CIT), chemotherapy (CT), immunotherapy (IT), ibr, and other novel agents. For this interim analysis (data cut: Feb 2018), the number of pts with CLL who had testing performed for FISH, TP53 mutational status, and IGHV mutational status, as well as CLL tx for subgroups of pts stratified by abnormality, was summarized as frequency counts and percentages.
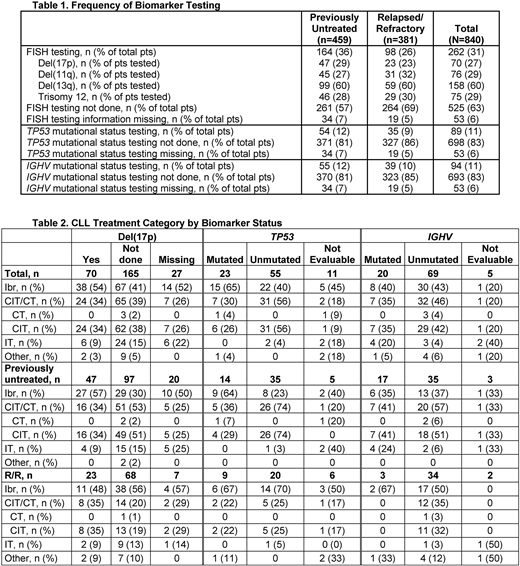
Results: At the time of this analysis, the registry had enrolled 840 pts (459 previously untreated; 381 relapsed or refractory [R/R]). The majority of pts were male (64%) and Caucasian (92%); median (range) age was 70y (34-95), and median (range) Charlson Comorbidity Index was 2 (0-9). Overall, prognostic biomarker testing was performed infrequently. Among all pts (N=840), 262 (31%) had FISH testing, 89 (11%) had testing performed for TP53 mutation, and 94 (11%) had testing for IGHV mutational status (Table 1). Among 459 pts tested prior to first-line tx, 164 (36%) had testing for FISH, 54 (12%) for TP53, and 55 (12%) for IGHV; among 381 R/R pts, 98 (26%) had testing for FISH, 35 (9%) for TP53, and 39 (10%) for IGHV. For tested pts, 70/262 (27%) pts had del(17p), 23/89 (26%) had mutated TP53, and 69/94 (73%) had U-CLL. For previously untreated tested pts, 47/164 (29%) had del(17p), 14/54 (26%) had mutated TP53, and 35/55 (64%) had U-CLL; for tested R/R pts, 23/98 (23%) had del(17p), 9/35 (26%) had mutated TP53, and 34/39 (87%) had U-CLL. Among 70 pts with del(17p), the most common tx was ibr (n=38; 54%); however, a considerable proportion of pts received CT/CIT (n=24; 34%) (Table 2). In 47 previously untreated pts with del(17p), 27 (57%) received ibr and 16 (34%) received CT/CIT; in 23 R/R pts with del(17p), 11 (48%) received ibr and 8 (35%) CT/CIT. Among 23 pts with mutated TP53, 15 (65%) were treated with ibr, while 7 (30%) with CT/CIT. Of 14 previously untreated pts with mutated TP53, 9 (64%) received ibr and 5 (36%) CT/CIT; of 9 R/R pts with mutated TP53, 6 (67%) received ibr and 2 (22%) CT/CIT. Among 69 pts with U-CLL, 30 (43%) were treated with ibr and 32 (46%) with CT/CIT. In 35 previously untreated pts with U-CLL, CT/CIT was more common (n=20; 57%) than ibr (n=13; 37%), while in 34 R/R pts with U-CLL, ibr was more common (n=17; 50%) than CT/CIT (n=12; 35%).
Conclusions: There remains a considerable lack of prognostic marker testing among pts with CLL in the modern era. These findings, as compared to prior registry results, suggest that the advent of novel agents and specific testing guidelines (eg, iwCLL) have not improved prognostic testing patterns in the real-world setting. Moreover, of pts tested who had abnormalities such as del(17p), TP53 mutation, or U-CLL, approximately one-third still received CIT. These results underscore a need to educate on how to utilize these markers to guide CLL tx decisions for optimal clinical outcomes. Additional evaluations (eg, regression analyses) to identify factors associated with failure to perform FISH, TP53, and IGHV testing are planned.
Mato:Portola: Research Funding; Celgene: Consultancy; AstraZeneca: Consultancy; AbbVie: Consultancy, Research Funding; Medscape: Honoraria; TG Therapeutics: Consultancy, Research Funding; Prime Oncology: Honoraria; Regeneron: Research Funding; Johnson & Johnson: Consultancy; Acerta: Research Funding; Pharmacyclics, an AbbVie Company: Consultancy, Research Funding. Barrientos:Janssen: Consultancy; Gilead: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Pharmacyclics, an AbbVie Company: Consultancy, Research Funding. Brander:BeiGene: Other: Institutional research funding for non investigator initiated clinical trial, Research Funding; Genentech: Consultancy, Honoraria, Other: Institutional research funding for non investigator initiated clinical trial, Research Funding; Novartis: Consultancy, Other: DSMB; DTRM: Other: Institutional research funding for non investigator initiated clinical trial, Research Funding; Pharmacyclics, an AbbVie Company: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Other: Institutional research funding for non investigator initiated clinical trial, Research Funding; Teva: Consultancy, Honoraria; TG Therapeutics: Consultancy, Honoraria, Other: Institutional research funding for non investigator initiated clinical trial, Research Funding; Acerta: Other: Institutional research funding for non investigator initiated clinical trial, Research Funding. Pagel:Pharmacyclics, an AbbVie Company: Consultancy; Gilead: Consultancy. Kadish:Pharmacyclics, an AbbVie Company: Speakers Bureau; Celgene: Speakers Bureau; Janssen: Speakers Bureau; Takeda: Speakers Bureau. Ghosh:Celgene: Consultancy; PCYC: Consultancy, Research Funding, Speakers Bureau; Gilead: Consultancy, Speakers Bureau; Pharmacyclics, an Abbvie Company: Consultancy, Research Funding, Speakers Bureau; SGN: Consultancy, Research Funding, Speakers Bureau; Forty seven Inc: Research Funding; TG Therapeutics: Honoraria, Research Funding; F. Hoffman-La Roche Ltd: Research Funding; Genentech: Research Funding; Spectrum: Consultancy; Abbvie: Consultancy, Speakers Bureau; Juno: Consultancy, Research Funding. Giafis:Pharmacyclics, an AbbVie Company: Employment, Other: Travel; AbbVie: Equity Ownership. Ipe:AbbVie: Equity Ownership; Pharmacyclics, an AbbVie Company: Employment, Other: Travel. Upasani:Pharmacyclics, an AbbVie Company (self and immediate family member): Employment; AbbVie (self and immediate family member): Equity Ownership. Sundaram:AbbVie: Employment, Equity Ownership, Other: Travel; Johnson & Johnson: Employment, Equity Ownership, Other: Travel. Ferrante:Janssen: Employment, Equity Ownership. Amaya-Chanaga:AbbVie: Equity Ownership, Other: Research performed while employed as an investigator of this study at UCSD. Review and approval of abstract performed while employed at Pharmacyclics, LLC, an AbbVie Company.; Pharmacyclics, an AbbVie Company: Employment, Other: Research performed while employed as an investigator of this study at UCSD. Review and approval of abstract performed while employed at Pharmacyclics, LLC, an AbbVie Company.. Iyengar:Pharmacyclics, an AbbVie company: Employment; AbbVie: Equity Ownership; Express Scripts: Patents & Royalties. Sharman:Acerta: Consultancy, Research Funding; Pharmacyclics, an AbbVie Company: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal