

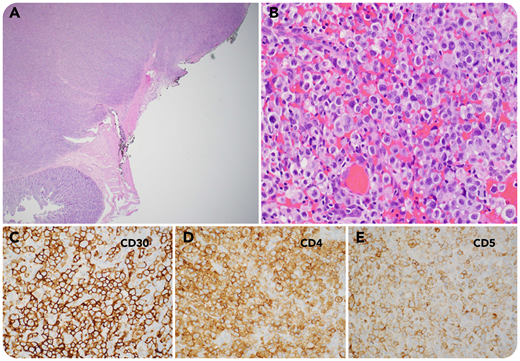
A 34-year-old man with a 3-month history of HIV (CD4, 191 cells per µL) presented to the emergency department with worsening intermittent abdominal pain, black stools, and night sweats for 1 week. A computed tomography scan showed continued intussusception in the jejunum. Exploratory laparotomy with small bowel resection was performed. Multiple masses (up to 3 cm) were noted in the ileum and jejunum, with full thickness involvement on gross examination (panel A; 2× objective; hematoxylin and eosin stain). Histology showed sheets of large anaplastic tumor cells involving both the small bowel and regional lymph nodes (panel B; 40× objective; hematoxylin and eosin stain). By immunohistochemistry (panels C-E; 40× objective), these cells were positive for CD30, CD4, CD5, CD2, CD7, granzyme B, perforin, and TIA-1 and negative for CD3, CD8, ALK1, EMA, HHV-8, LMP1, CD15, CD20, PAX5, CD138, and CD56, with EBER negativity by in situ hybridization (ISH). By fluorescence ISH, the cells were negative for DUSP22 and TP63 gene rearrangement. This case represented HIV-associated ALK− anaplastic large cell lymphoma (ALCL) without DUSP22 or TP63 gene rearrangement.
HIV-associated ALCL is rare, with ALK negativity and occurring almost exclusively with extranodal involvement and predominantly in young men. Our patient was recently diagnosed with AIDS, without prior AIDS-defining illnesses, with ALK− ALCL with a unique presentation of small bowel intussusception and also both extranodal and nodal involvement.
A 34-year-old man with a 3-month history of HIV (CD4, 191 cells per µL) presented to the emergency department with worsening intermittent abdominal pain, black stools, and night sweats for 1 week. A computed tomography scan showed continued intussusception in the jejunum. Exploratory laparotomy with small bowel resection was performed. Multiple masses (up to 3 cm) were noted in the ileum and jejunum, with full thickness involvement on gross examination (panel A; 2× objective; hematoxylin and eosin stain). Histology showed sheets of large anaplastic tumor cells involving both the small bowel and regional lymph nodes (panel B; 40× objective; hematoxylin and eosin stain). By immunohistochemistry (panels C-E; 40× objective), these cells were positive for CD30, CD4, CD5, CD2, CD7, granzyme B, perforin, and TIA-1 and negative for CD3, CD8, ALK1, EMA, HHV-8, LMP1, CD15, CD20, PAX5, CD138, and CD56, with EBER negativity by in situ hybridization (ISH). By fluorescence ISH, the cells were negative for DUSP22 and TP63 gene rearrangement. This case represented HIV-associated ALK− anaplastic large cell lymphoma (ALCL) without DUSP22 or TP63 gene rearrangement.
HIV-associated ALCL is rare, with ALK negativity and occurring almost exclusively with extranodal involvement and predominantly in young men. Our patient was recently diagnosed with AIDS, without prior AIDS-defining illnesses, with ALK− ALCL with a unique presentation of small bowel intussusception and also both extranodal and nodal involvement.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal