

TO THE EDITOR:
Inhibitory antibodies (inhibitors) against factor VIII (FVIII) develop in 25% to 35% of previously untreated patients (PUPs) with severe hemophilia A (SHA). It is the most serious complication of classic hemophilia treatment.1-3 Most inhibitors develop during the first 50 exposure days (EDs) to FVIII, with 50% of inhibitors already present after 14 to 15 EDs.2-4 After 50 EDs, inhibitor development is rare and is reported in number of new inhibitors per 1000 person-years. A recent systematic review reported an overall inhibitor incidence of 2.06 per 1000 person-years.5 A definition specifically designed to separate a priori high-risk and low-risk category patients was established after the outbreaks of 2 product-specific inhibitors in the 1990s.6-8 According to this definition, previously treated patients (PTPs), considered tolerant to exogenous FVIII, are patients with >150 EDs.8
Hemophilia treatment has changed considerably over the last decades due to the development of many new therapies.9 Prophylaxis, first only practiced in a few countries, has become standard of care and is started at increasingly earlier ages and with higher dosing and frequencies.10,11
The PedNet cohort study prospectively includes all newly diagnosed patients with hemophilia of the participating centers.12
The aim of this study was to define the risk periods for inhibitor development until 1000 EDs and to refine the definition of PTPs and the age at which patients have reached this “near-zero” risk situation.
All PUPs with SHA (FVIII activity <0.01 IU/mL) born from 1 January 2000 onward, and diagnosed in 1 of the participating centers of the PedNet Study Group (supplemental Appendix, available on the Blood Web site), were enrolled into the PedNet study protocol (this trial was registered at www.clinicaltrials.gov as #NCT02979119). The study design is an unselected birth cohort that included over 90% of all newly diagnosed patients in the participating centers. Detailed data on each ED was collected until 75 EDs for patients born between 2000 and 2009 and until 50 EDs for patients born from 2010 onward. Approval for inclusion in the registry was obtained from every center’s institutional review board. Written informed consent was obtained from the parents/guardians of all participants.
For the present analysis, patients were followed until inhibitor development, or censored based on the number of EDs at their last follow-up as of January 2018.
The primary outcome of the study was development of a clinically relevant inhibitor, defined as at least 2 positive inhibitor titers in combination with decreased in vivo FVIII recovery. The secondary outcome was development of a high-titer inhibitor, defined as the occurrence of a clinically relevant inhibitor with a peak titer of at least 5 Bethesda units (BU)/mL. Positivity was defined according to the cutoff level in each individual center’s laboratory, the highest cutoff level used being 0.6 BU/mL. The number of EDs at the time of inhibitor development was defined as the last ED before the first positive titer was reported. All laboratory results for inhibitor tests in all patients were collected.
To calculate cumulative inhibitor incidence according to the number of EDs, survival analysis was performed with EDs up to 1000 as the time variable. We calculated the median age and interquartile range (IQR) in years at ED 1 and ED 75. To assess inhibitor rate in person-years, we included all patients who had reached 75 EDs and calculated the time in years between the date of ED 75 and the date of their last follow-up. Analyses were performed using SPSS 24.
A total of 1038 PUPs with SHA were eligible, 943 of whom (91%) were followed until 50 EDs; 899 (87%) were followed until 75 EDs (Table 1). The median (IQR) age at first exposure was 1.1 years (0.8-1.5 years); 75 EDs were reached at a median (IQR) age of 2.3 years (1.7-2.8 years), only 1.2 years after the first ED. A total of 869 patients (83.7%) were of white ancestry. Almost all inhibitors (298 of 300; 99.3%) developed within the first 75 EDs. Seventy-nine percent of all inhibitors (N = 236, 173 high-titer and 63 low-titer) developed within 20 EDs, 18% (N = 53, 35 high-titer and 18 low-titer) between 21 and 50 EDs, and 3% (N = 9, 4 high-titer and 5 low-titer) between 51 and 75 EDs (Table 1).
Inhibitor development from ED 1 until 1000 EDs for all and high-titer inhibitors
| EDs | Patients at risk | Patients with inhibitors | High-titer inhibitors | All inhibitors, cumulative % |
|---|---|---|---|---|
| 0 | 1038 | 0 | 0 | 0 |
| 1-10 | 897 | 109 | 78 | 36 |
| 11-20 | 753 | 236 | 173 | 79 |
| 21-30 | 708 | 268 | 196 | 89 |
| 31-40 | 688 | 282 | 203 | 94 |
| 41-50 | 654 | 289 | 208 | 96 |
| 51-60 | 646 | 294 | 210 | 98 |
| 61-75 | 601 | 298 | 212 | 99.3 |
| 76-150 | 568 | 298 | 212 | 99.3 |
| 151-250 | 524 | 299 | 212 | 99.7 |
| 251-500 | 430 | 300 | 212 | 100 |
| 501-1000 | 214 | 300 | 212 | 100 |
| EDs | Patients at risk | Patients with inhibitors | High-titer inhibitors | All inhibitors, cumulative % |
|---|---|---|---|---|
| 0 | 1038 | 0 | 0 | 0 |
| 1-10 | 897 | 109 | 78 | 36 |
| 11-20 | 753 | 236 | 173 | 79 |
| 21-30 | 708 | 268 | 196 | 89 |
| 31-40 | 688 | 282 | 203 | 94 |
| 41-50 | 654 | 289 | 208 | 96 |
| 51-60 | 646 | 294 | 210 | 98 |
| 61-75 | 601 | 298 | 212 | 99.3 |
| 76-150 | 568 | 298 | 212 | 99.3 |
| 151-250 | 524 | 299 | 212 | 99.7 |
| 251-500 | 430 | 300 | 212 | 100 |
| 501-1000 | 214 | 300 | 212 | 100 |
The cumulative inhibitor incidence for all inhibitors is reported during follow-up.
At this point, inhibitor development reached a plateau. No inhibitors developed between 75 and 150 EDs, whereas another 2 low-titer inhibitors (0.7%) developed at ED 249 and 262 EDs, respectively (Figure 1). Based on survival analysis, the cumulative inhibitor incidence was 28.9% at 50 EDs and 29.9% at 75 EDs. Total cumulative inhibitor incidence reached 30.2% at 1000 EDs (Table 1).
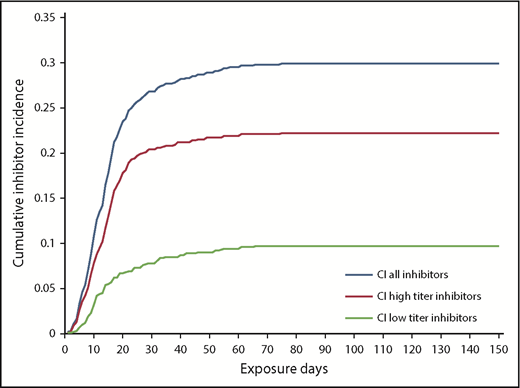
Kaplan-Meier curve of 1038 patients with SHA followed from ED 1 onward until ED 150. After 75 EDs, only 2 low-titer inhibitors developed, at 249 and 264 EDs.
Kaplan-Meier curve of 1038 patients with SHA followed from ED 1 onward until ED 150. After 75 EDs, only 2 low-titer inhibitors developed, at 249 and 264 EDs.
In newborns with severe hemophilia A, inhibitor development is of great concern to parents and physicians. Knowing the time period of greatest risk is important as there is evidence that intense exposure to FVIII (as occurs with surgery) should be avoided during this period as this might increase the inhibitor risk.2,13,14 Our study shows that children on prophylaxis reach a near-zero risk plateau of inhibitor development at 75 EDs only 1.2 years after the first ED.
We were interested in determining inhibitor risk after 75 EDs. To calculate this, we included all patients who reached at least 75 EDs and calculated the time between the date of ED 75 and the date of last follow-up. The total follow-up time was 4031 person-years. Because only 2 low-titer inhibitors occurred in this period, the calculated inhibitor risk was only 0.5 per 1000 person-years. Earlier studies reported much higher risks for PTPs. In 1 of the first studies, a 4-year prospective study from the United States, 31 new inhibitors were detected in 1306 patients. The study concluded that inhibitor risk was 8 per 1000 person-years; this risk was used as an estimate to evaluate neoimmunogenicity in new products.15 However, that study included patients with <50 EDs (ie, PUPs), causing the denominator to be a mixture of PTPs and PUPs. Studies reporting only on PTPs (using the definition of >150 EDs) over the last decades estimated the inhibitor risk at ∼2 to 4 per 1000 person-years.4,5,16,17
Recently, investigators suggested that clinical trials in PUPs at 20 EDs be stopped, arguing that most inhibitors develop very early, whereas longer follow-up was too time-consuming and limited by patients being lost to follow-up.18 Our data on 1038 PUPs with SHA show that such an approach would be inappropriate, as 21% of inhibitors occurred between 21 and 75 EDs. Clinical trials of factor concentrates in PUPs undertaken by manufacturers have generally followed patients only until 50 EDs or until 3 years on study. Differences in follow-up period and, as a consequence, the lack of information regarding late inhibitors have beenimportant limitations in comparing inhibitor risks between studies.19,20 Our data demonstrate that the age to reach 75 EDs was at a median of 2.3 years. Frequent testing for inhibitors until 75 instead of 50 EDs, therefore, is feasible and should be recommended for all PUPs.
It should be noted that our results are applicable to children who receive early prophylaxis, as almost all of our patients were started on prophylaxis very early in life.11 In countries where this is not the case, the timing of inhibitor development could potentially be different.
In conclusion, we have strong evidence from the largest prospective cohort study of PUPs that virtually all inhibitors develop by ED 75. Consequently, we propose that 75 EDs should to be the cutoff to distinguish PUPs from PTPs.
Data collected in the frame work of the PedNet cohort studies are available for all members of the PedNet study group.
The online version of this article contains a data supplement.
Acknowledgments
The authors thank all of the data registrars of the PedNet Study Group for providing data, and Ella van Hardeveld and Marloes de Kovel for managing data, verifying sources, and running quality checks.
Authorship
Contribution: All authors were members of the writing committee.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
A complete list of the members of the PedNet Study Group appears in the supplemental Appendix, available on the Blood Web site.
Correspondence: H. Marijke van den Berg, PedNet Haemophilia Research Foundation, Mollerusstraat 1, 3743 BW Baarn, The Netherlands; e-mail: h.marijke.vandenberg@pednet.eu.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal