

INTRODUCTION: A massive transfusion protocol (MTP) is defined as a transfusion which exceeds the patient's estimated blood volume within 24 hours. The use of cold-stored, low-titer Group O whole blood (LTOWB) is well established for massive transfusion in military and civilian trauma. However, we do not yet have data supporting the use of LTOWB for non-trauma patients requiring a massive transfusion. Herein lies the importance of this retrospective cohort study as it seeks to answer important questions about the use of LTOWB in non-trauma patients. The primary aim of the study is to establish if mortality 24h and 30d after LTOWB MTP is no worse than after standard, component MTP. Secondary aims include degree of hemolysis, length of stay and, because there is 5% increase in mortality for every minute that blood products are not provided to a trauma patient after an MTP has been activated, time to delivery.
METHODS: A retrospective chart review identified non-trauma patients requiring a MTP from July 1, 2018 to June 30, 2019, comparing those who received at least one unit of LTOWB ("LTOWB" cohort) to those who received a standard component MTP ("Component" cohort). Each delivery of a component MTP contains 6u of RBCs, 6u of plasma and 1u of platelets. Each LTOWB delivery contains 5u of leukoreduced (using a platelet-sparing filter) LTOWB. Our primary outcomes were 24h and 30d mortality, adjusted for age and Elixhauser comorbidity score. Secondary outcomes included length of stay, hemolysis, and delivery time.
Medical records were abstracted for demographics, Total Bilirubin levels, discharge codes, 24h and 30d mortality, and length of stay. Hemolysis was the difference between highest Total Bilirubin in the 5 days following the MTP and the lowest total bilirubin level for the two days prior or on the day of the MTP. Delivery time was calculated as the number of minutes between the time the MTP was ordered in the electronic ordering system and the delivery of the first box of blood products as noted in hospital transportation logs. Discharge codes were used to calculate a weighted Elixhauser comorbidity score as previously described. Statistical analysis was performed utilizing logistic regressions, poisson regression, general linear models, and t-tests as appropriate (Table 2, Table 3).
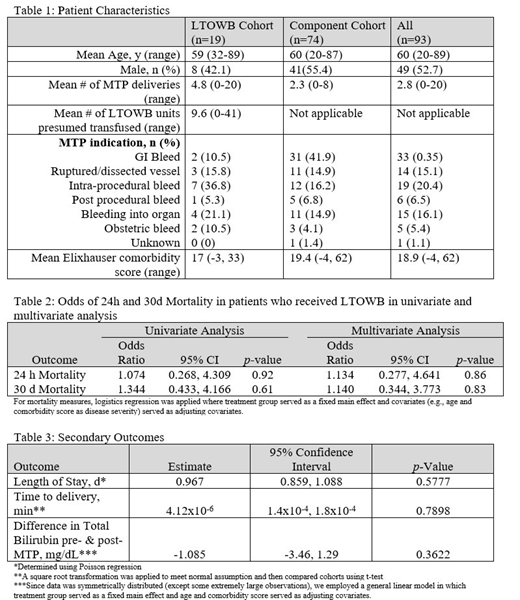
RESULTS: Between 7/1/2018 and 6/30/2019, 93 unique patients received 114 MTPs, of which 19 received at least one unit of LTOWB (Table 1). Seven patients had emergency-issue blood delivered outside of hospital transportation so were included in the analysis. The indication for the MTP was most commonly gastrointestinal bleeding, followed by intra-procedural bleeding and organ bleeding (spleen, pancreas, retroperitoneum, lung, brain and ovarian). Adjusting for age and Elixhauser comorbidity score, there was no statistically significant difference in 24 h mortality (13.4% higher odds in LTOWB cohort compared to component; 95% confidence interval (CI): 0.28, 4.64; p: 0.86) or 30 d mortality (14% higher odds in LTOWB cohort compared to component; 95% CI: 0.34, 3.77; p: 0.83), Table 2. There was no statistically significant difference between cohorts in length of stay (for every 1.0 day patients who received LTOWB were admitted, patients who received components were admitted for 0.97d; 95% CI: 0.86, 1.09; p: 0.58), time to delivery, or degree of hemolysis.
CONCLUSIONS: For non-trauma patients receiving a massive transfusion, our data suggest that receiving at least one unit of LTOWB does not impact 24 h or 30 d mortality. Length of stay and change in bilirubin were nearly the same for both cohorts suggesting that LTOWB is as safe as component therapy. Although we hypothesized that LTOWB would be delivered faster, we have a small sample size and because component MTP is the default at our institution for non-trauma patients, LTOWB was usually delivered only in subsequent deliveries, not the first one. Therefore, we would not expect to see a difference. Although this is a small study from one institution, it is the first investigation of LTOWB in non-trauma patients. Overall, our data indicates that LTOWB may be a reasonable alternative to component therapy outside of trauma as it does not significantly alter patient outcomes but still eases manufacturing and transfusion logistics. Future research is needed to further establish the effects of LTOWB in this population.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal