

Purpose: Hodgkin's lymphoma (HL) is a highly curable disease even in advanced-stage, with >90% of long-term survivors. Currently, the standard of care is ABVD (doxorubicin, etoposide, vinblastine and dacarbazine), as it is less toxic and as effective as other more intensive chemotherapy regimens. Alternatively, BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine and prednisone) has been proposed as front-line intensified regimen with a better initial disease control and prolonged time to relapse when compared to ABVD. However, this advantage is associated with higher rates of severe hematologic toxicity, treatment-related deaths, secondary neoplasms and infertility. To date, the debate regarding which regimen should be preferred as first line for advanced-stage HL is still ongoing. To shed some light on this open question we compared efficacy and safety of both regimens in clinical practice.
Patients and Methods: From October 2009 to October 2018, patients with HL stage III-IV treated with either ABVD or BEACOPP escalated (BEACOPPesc) were retrospectively assessed in 7 European cancer centers.
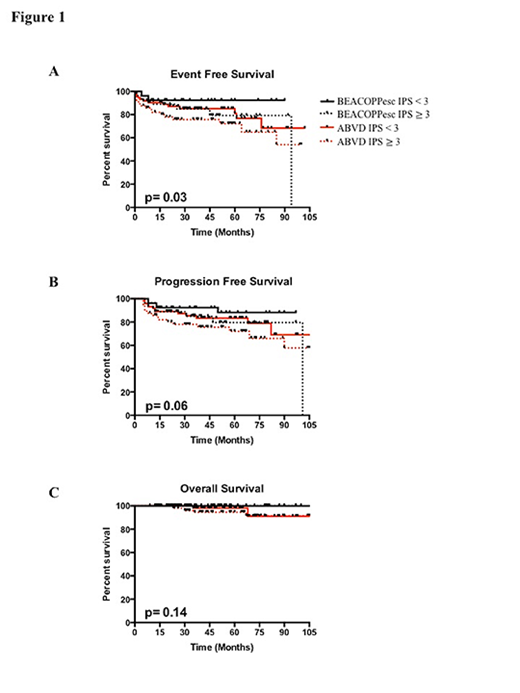
Results: A total of 372 consecutive patients were included in the study. One-hundred and ten patients were treated with BEACOPPesc and 262 with ABVD. The baseline characteristics of the two groups did not differ significantly, except for a higher rate of high-risk patients in the BEACOPPesc group in contrast to the ABVD one (47% vs 18%; p= 0.003). Complete response rate (CR) assessed by PET imaging at the end of the second cycle was 67% and 78% for the ABVD and BEACOPPesc group (p= 0.003), respectively. Thirteen patients of the ABVD group achieved stable disease (SD) and 6 had a progression disease (PD). On the other hand, 4 of the patients in the BEACOPPesc group progressed, another 2 interrupted therapy because life-threatening toxicity. At the end of the therapy, CR was 76% in the ABVD group and 85% in the BEACOPPesc group (p= 0.01). A total of 20% patients in the ABVD group and 14% patients in the BEACOPPesc group received consolidation radiotherapy on the mediastinal mass at the dose of 30Gy. After radiotherapy, the number of patients with CR increased to 79% and 87% in the two groups (p= 0.041), respectively. Thirty-nine patients (35%) in the BEACOPPesc group required dose reduction of chemotherapy due to toxicity compared to 12 patients (5%; p= <0.001) in the ABVD group. Overall, the rate of severe toxicities was higher in the BEACOPPesc group in comparison with the ABVD cohort. In particular, there was a significant increased frequency of acute grade 3-4 hematologic adverse events (neutropenia 61% vs 24%; anemia 29% vs 4%; thrombocytopenia 29% vs 3%), febrile neutropenia (29% vs 3%), severe infections (18% vs 3%). Myeloid growth factors were administered to 85% and 59% of patients in the BEACOPPesc group compared to the ABVD group. Blood transfusions were required in 51% and 6% of patients in the BEACOPPesc group compared to the ABVD cohort. Progression during or shortly after treatment occurred in 5 patients in the BEACOPPesc group (4%) and in 16 patients in the ABVD group (6%; p= 0.62). Among the 96 patients who achieved a CR after BEACOPPesc and radiotherapy, 8 relapsed (8%), compared to 29 of 208 patients in the ABVD group (14%; p= 0.04). At a median follow-up period of 5 years, no statistical difference in progression free survival (PFS; p=0.11) and event-free survival (EFS; p=0.22) was observed between the BEACOPPesc and ABVD cohorts. Similarly, overall survival (OS) did not differ between the two groups (p=0.14). The baseline international prognostic score (IPS <3 vs ≥ 3) significantly influenced the EFS with an advantage for the high-risk group treated with BEACOPPesc (Figure 1A; p=0.03), but not the PFS (Figure 1B; p=0.06) and OS (Figure 1C; p=0.14). During the follow-up period, in the BEACOPPesc group one patient developed myelodysplasia and one acute leukemia. Second solid tumors developed in one patient in the ABVD group (lung cancer) and one in BEACOPPesc group (breast cancer).
Conclusion: We confirm that the ABVD regimen is an effective and less toxic therapeutic option for advanced-stage HL. Although BEACOPP results in better initial tumor control especially in high-risk patients, the long-term outcome remains similar between the two regimens.
Ferrero:EUSA Pharma: Membership on an entity's Board of Directors or advisory committees; Servier: Speakers Bureau; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead: Speakers Bureau. Martinelli:BMS: Consultancy; Pfizer: Consultancy; ARIAD: Consultancy; Roche: Consultancy; Novartis: Consultancy. Willenbacher:European Commission: Research Funding; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Myelom- und Lymphomselbsthilfe Österreich: Consultancy, Honoraria; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Gilead Science: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; IQVIA: Membership on an entity's Board of Directors or advisory committees; Merck: Consultancy, Membership on an entity's Board of Directors or advisory committees; oncotyrol: Employment, Research Funding; Bristol-Myers Squibb: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Fujimoto: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Tirol Program: Research Funding; Abbvie: Consultancy, Honoraria; Sandoz: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal