

Background: Two commercial anti-CD19 chimeric antigen receptor T-cell therapies (CART19) are currently approved by the FDA for r/r aggressive B-cell lymphomas: axicabtagene ciloleucel (approved in October 2017) and tisagenlecleucel (tisa-cel, approved in May 2018). In published clinical trials, CART19 therapy results in long term remissions in 30-40% of patients (pts). While most CART19 protocols use cyclophosphamide/fludarabine (Cy/Flu) for lymphodepleting chemotherapy (LDC) prior to CART19 infusion, the phase 2 JULIET trial (NCT02445248) with tisa-cel allowed investigator's choice of Cy/Flu or bendamustine. LDC was not required for pts with WBC <1000 cells/μL within one week prior to tisa-cel infusion. In JULIET, 75 (73%) pts received Cy/Flu, 21 (20%) pts received bendamustine, and 7 (7%) pts received no LDC (Schuster et al, NEJM 2019). Grade 3 or 4 cytopenias not resolved by Day 28 following tisa-cel included thrombocytopenia (40%) and neutropenia (25%) among JULIET pts (FDA package insert). Many r/r lymphoma pts are Cy-resistant and bendamustine is not cross-resistant with Cy. Prolonged cytopenias can be seen with Cy/Flu in addition to lymphopenia. In an effort to reduce tumor volume and minimize cytopenias, bendamustine is frequently used for LDC at our institution. We report our experience with bendamustine as LDC before commercially supplied tisa-cel.
Methods: We conducted a single center, retrospective, IRB-approved analysis of r/r lymphoma pts receiving commercial tisa-cel at the University of Pennsylvania. Responses were based on treating physician's assessment utilizing Revised Response Criteria for Malignant Lymphoma (Cheson et al, JCO 2014). Unless the pt had signs or symptoms of progressive lymphoma, response assessment was generally performed at 3 months from tisa-cel infusion per our institutional practice and based on evidence that 3-month response outcomes are more predictive of long-term efficacy than 1-month outcomes. Cytokine release syndrome (CRS) was assessed using Penn criteria (Porter et al, J Hematol Oncol 2018). Neurotoxicity was graded using CARTOX-based scale (Neelapu et al, Nat Rev Clin Oncol 2018). Cytopenias were graded using Common Terminology Criteria for Adverse Events, version 5.
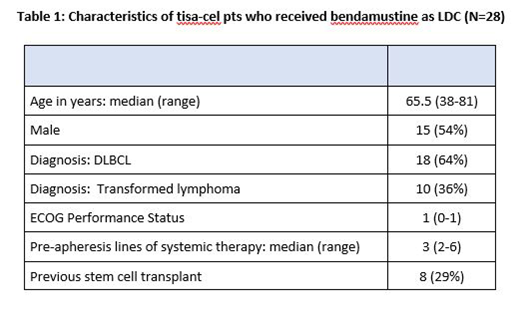
Results: We identified 28 pts with DLBCL or transformed lymphoma who received commercially supplied tisa-cel between June 2018 and June 2019 with bendamustine as LDC and a follow-up of at least 30 days from the infusion. Pt characteristics are described in Table 1. Median age was 65.5 years (range: 38-81). Bendamustine dose was 90 mg/m2 intravenously daily for 2 days in 23/28 (82%) pts with remaining 5/28 (18%) pts receiving lower doses at the discretion of the treating physician.
Twenty-four of 28 pts received bendamustine for LDC and had at least 3-month follow-up or progression prior to 3 months. The 3-month overall response rate was 11/24 (46%) with complete response rate 9/24 (38%). With median follow-up 5.5 months, 3-month progression-free survival estimate was 52% (95%CI: 30%-70%). In terms of toxicities in this cohort, there were no deaths related to tisa-cel. CRS was experienced by 8/28 (29%) of pts with no grade 3 or 4 events by Penn scale. Neurotoxicity was seen in 2/28 (7%) pts with 1 (4%) experiencing transient grade 3 by CARTOX-based grading. At day 28 post tisa-cel infusion, 3/28 (11%) pts had grade 3 or higher neutropenia and 3/28 (11%) had grade 3 or higher thrombocytopenia. Most pts were treated as outpatients with only 2/28 (7%) receiving tisa-cel infusion as inpatient.
Conclusion: Three-month complete response rates are considered reasonably predictive of outcome for CART19 therapies. Although our follow-up is short, our experience shows that bendamustine as LDC for tisa-cel performs well outside of a clinical trial, is an option for LDC before tisa-cel therapy for pts with r/r aggressive B-cell lymphomas treated in the outpatient setting, and may have an improved safety profile with regard to cytopenias.
Svoboda:Kyowa: Consultancy; Merck: Research Funding; BMS: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; AstraZeneca: Consultancy; Celgene: Research Funding; Incyte: Research Funding; Pharmacyclics: Consultancy, Research Funding. Chong:Novartis: Consultancy; Merck: Research Funding; Tessa: Consultancy. Hughes:Genzyme: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Acerta Pharna/HOPA: Research Funding. Dwivedy Nasta:Millenium/takeda: Research Funding; Debiopharm: Research Funding; Aileron: Research Funding; ATARA: Research Funding; Pharmacyclics: Research Funding; Celgene: Honoraria; Merck: Consultancy, Other: data safety monitorin; 47 (Forty Seven): Research Funding; Roche: Research Funding; Rafael: Research Funding. Landsburg:Celgene: Membership on an entity's Board of Directors or advisory committees; Triphase: Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Seattle Genetics: Speakers Bureau; Seattle Genetics: Speakers Bureau; Curis, INC: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Research Funding; Triphase: Research Funding; Takeda: Research Funding. Barta:Bayer: Consultancy, Research Funding; Celgene: Research Funding; Mundipharma: Honoraria; Janssen: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding; Seattle Genetics: Honoraria, Research Funding; Mundipharma: Honoraria; Merck: Research Funding; Celgene: Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees. Gerson:Abbvie: Consultancy; Seattle Genetics: Consultancy; Pharmacyclics: Consultancy. Ruella:Novartis: Patents & Royalties: CART for cancer; AbClon: Membership on an entity's Board of Directors or advisory committees; Nanostring: Consultancy, Speakers Bureau. Frey:Novartis: Research Funding. Porter:Novartis: Membership on an entity's Board of Directors or advisory committees, Patents & Royalties, Research Funding; Kite: Membership on an entity's Board of Directors or advisory committees; Glenmark Pharm: Membership on an entity's Board of Directors or advisory committees; Immunovative: Membership on an entity's Board of Directors or advisory committees; American Board of Internal Medicine: Membership on an entity's Board of Directors or advisory committees; Genentech: Employment; Wiley and Sons: Honoraria; Incyte: Membership on an entity's Board of Directors or advisory committees. Schuster:Nordic Nanovector, Pfizer, AstraZeneca, Loxo Oncology, Acerta, and Celgene: Honoraria; Novartis, Celgene, Genentech, Merck, Pharmacyclics, Acerta, and Gilead: Other: Grants, Research Funding; Novartis: Other: a patent (with royalties paid to Novartis) on combination therapies of CAR and PD-1 inhibitors.; Novartis, Nordic Nanovector, and Pfizer: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal