

Background: A variety of risk factors have been described in multiple myeloma and current risk assessment incorporates ISS stage with specific FISH results and serum LDH (R-ISS). However, this model does not include all the current abnormalities described as prognostic for survival in multiple myeloma. Importantly, the impact of many of these high-risk abnormalities are not uniform. We examined if we can better integrate FISH results into a risk assessment tool to better predict the outcomes of newly diagnosed MM.
Patients and methods: We studied a cohort of 1316 patients with FISH done within 6 months of diagnosis of MM, in whom results for commonly observed abnormalities were available. We specifically examined the individual impact of common translocations involving chromosome 14, MYC rearrangements, chromosome 1q gain (single or multiple duplication) and del13q/monosomy 13. A risk assessment system was developed, weighting each abnormality according to their Risk Ratio and integrating ISS stage and serum LDH into the final model construction. Overall survival was calculated from diagnosis, with those alive at last follow up being censored.
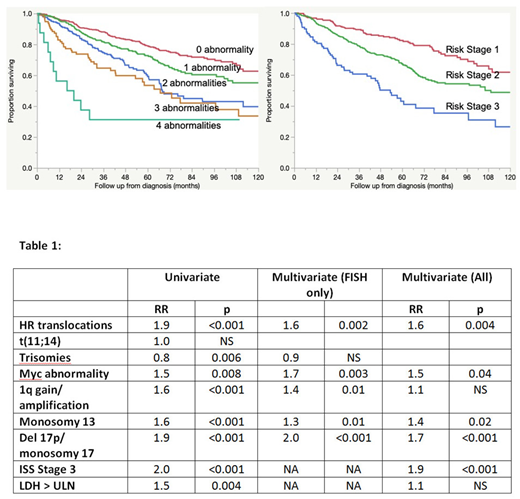
Results: We first examined the impact of each of the above FISH abnormalities: 1) high risk translocations [t(4;14), t(14;16), or t(14,20)], 2) trisomies, 3) t(11;14), 4) MYCrearrangements, 5) del13q/monosomy 13, and 6) 1q gain . Each of the abnormalities, except for t(11;14), was prognostic for survival (Table 1 with the risk ratios). For 1q gain, the median OS was NR, 105 mos and 79 mos respectively for no abnormality, duplication of 1 copy and duplication of multiple copies, (p<0.001). On multivariate analysis, t(11;14) and trisomies were no longer prognostic for overall survival (Table 1). The cumulative impact of abnormalities demonstrated worsening survival in the presence of increasing numbers of abnormalities (Figure 1). Including ISS stage 3 and LDH > ULN as additional variables for prognostication indicated both were individually prognostic for OS. In a multivariate analysis, including these two and FISH abnormalities, 1q gain and LDH were not independently prognostic. The final model consisted of HR translocations, MYCrearrangements, del17p/monosomy 17, del13q/monosomy 13, and ISS stage 3. Each of these variables was weighted using their risk ratio and a composite score was developed using 998 patients for whom all variables were available (range: 0-7.9; median 1.8). Three patient groups were characterized: group 1 (0; 32%), group 2 (1-4; 58%) and group 3 (>4; 10%) with a median OS of 53 mos, 106 mos, and NR, respectively, p <0.001 (Figure 2).
Conclusion: Using the most relevant FISH and laboratory factors, in a large cohort of patients, we refined the current system to develop a risk stratification system that predicts survival in patients with newly diagnosed MM treated with contemporary treatment regimens. This needs validation in future studies.
Kumar:Janssen: Consultancy, Research Funding; Takeda: Research Funding; Celgene: Consultancy, Research Funding. Gertz:International Waldenstrom Foundation: Research Funding; Annexon: Consultancy; Medscape: Consultancy, Speakers Bureau; Amyloidosis Foundation: Research Funding; Abbvie: Other: personal fees for Data Safety Monitoring board; i3Health: Other: Development of educational programs and materials; Springer Publishing: Patents & Royalties; Physicians Education Resource: Consultancy; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Proclara: Membership on an entity's Board of Directors or advisory committees; Ionis/Akcea: Consultancy; Alnylam: Consultancy; Prothena Biosciences Inc: Consultancy; Celgene: Consultancy; Janssen: Consultancy; Spectrum: Consultancy, Research Funding; Appellis: Consultancy; Research to Practice: Consultancy; Teva: Speakers Bureau; Johnson and Johnson: Speakers Bureau; DAVA oncology: Speakers Bureau; Amgen: Consultancy. Dispenzieri:Akcea: Consultancy; Janssen: Consultancy; Intellia: Consultancy; Pfizer: Research Funding; Takeda: Research Funding; Celgene: Research Funding; Alnylam: Research Funding. Lacy:Celgene: Research Funding. Dingli:alexion: Consultancy; Janssen: Consultancy; Millenium: Consultancy; Rigel: Consultancy; Karyopharm: Research Funding. Kapoor:Celgene: Honoraria; Janssen: Research Funding; Sanofi: Consultancy, Research Funding; Glaxo Smith Kline: Research Funding; Takeda: Honoraria, Research Funding; Amgen: Research Funding; Cellectar: Consultancy. Leung:Prothena: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding; Omeros: Research Funding; Aduro: Membership on an entity's Board of Directors or advisory committees. Bergsagel:Celgene: Consultancy; Ionis Pharmaceuticals: Consultancy; Janssen Pharmaceuticals: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal