

Background: Carfilzomib is effective in the treatment of relapsed and refractory multiple myeloma (RRMM). Questions remain regarding optimal dosing strategies and combinations. The MCRN-003/MYX.1 single arm phase II clinical trial of high-dose once weekly carfilzomib in combination with dexamethasone and cyclophosphamide (wCCD) in RRMM met its primary endpoint with an overall response rate (ORR) ≥ 80% after 4 treatment cycles [Venner, Blood 2018 132:1984]. This abstract focuses on previously unreported protocol specified secondary and exploratory endpoints including progression free (PFS) and overall survival (OS).
Methods: This multi-centre clinical trial is run through the Myeloma Canada Research Network (MCRN) with support from the Canadian Cancer Trials Group (CCTG). Patients who had 1-3 prior lines of therapy and without proteasome inhibitor (PI) refractory disease were eligible. Treatment consists of carfilzomib (20 mg/m2 day 1 of first cycle then escalated to 70 mg/m2 for all subsequent doses) given on days 1, 8, and 15 of a 28-day cycle, plus weekly oral dexamethasone 40 mg and cyclophosphamide 300 mg/m2 capped at 500 mg. Treatment continues until progression or intolerance, except for cyclophosphamide which is discontinued after 12 cycles.
Secondary endpoints included toxicity, depth of response, PFS and OS as defined by International Myeloma Working Group Uniform Response Criteria (2016). Exploratory endpoints included the impact of cytogenetics (CG) and prior PI or lenalidomide exposure on efficacy, and the novel endpoint of serum free light chain (sFLC) escape, defined as a > 25% change in the difference of involved to uninvolved light chain with the absolute rise > 100mg/L, in individuals with disease previously measurable by serum or urine protein electrophoresis. This analysis is based on the locked database of 19 June, 2019.
Results: Of 76 patients accrued, 75 were included in the analysis. One was ineligible due to prior bortezomib refractoriness. Thirty-nine percent received 1 prior line, 44% two prior lines and 17% three prior lines of therapy. High-risk cytogenetics (t(4;14), t(14;16) and/or del P53, considered positive at any level above local accepted threshold) were identified in 32%. Twenty percent had ISS stage III disease. The majority of participants were previously exposed to PI (87%) and lenalidomide (83%).
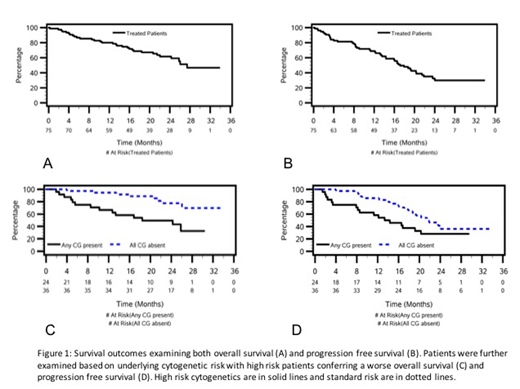
The median duration of follow-up was 25 months. The ORR at any time was 85% (1 patient achieved a response after 4 cycles) with ≥ VGPR achieved in 68% and ≥ CR in 29%. The presence of high-risk CG conferred a worse ORR (75% vs 97% respectively, p = 0.013). Thirty-one patients have died with a median OS and median PFS of 27 months and 17 months respectively (figure 1). High risk CG conferred a worse median OS (18 months vs NR, p = 0.002) and a trend toward a worse median PFS with high risk CG (14 months vs 22 months, p = 0.06; figure 1). For patients with prior PI exposure the median OS and PFS were 27 and 17 months respectively. For patients with prior lenalidomide exposure median OS and PFS were 26 and 16 months respectively. Free light chain escape events were noted in 11 patients (15%) but was the only progression event in 3 (4%). For the remaining 8 patients the sFLC rise was a harbinger of traditional relapse by electrophoresis. The median PFS when sFLC escape was included as a progression event was 17 months.
With updated toxicity data the most common ≥ grade 3 non-hematologic events were infection (40%), cardiac (15%, including 5 dyspnea and 1 pulmonary edema) and vascular (17%, including 7 with hypertension and 3 with thrombotic microangiopathy). To date 57 (76%) patients have discontinued carfilzomib, including 34 due to disease progression and 14 due to toxicity.
Conclusion: This phase II trial demonstrates that wCCD remains a safe and effective regimen for RRMM. The survival data presented here is comparable to current phase II and III studies examining the weekly dosing strategy. No new toxicity signals are observed but cardiovascular risks remain an important factor in the use of carfilzomib-based therapies. Using sFLC escape does not negatively affect PFS outcomes but likely better characterizes progression as a harbinger of more traditional events detected by electrophoresis. This regimen will be a useful triplet-based option for RRMM especially in patients refractory to lenalidomide and otherwise ineligible for the carfilzomib-lenalidomide-dexamethasone combination.
Venner:J&J: Research Funding. Leblanc:Amgen: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Sandhu:Takeda: Honoraria; Amgen: Honoraria; Celgene: Honoraria; Pfizer: Honoraria; Janssen: Honoraria; gilead: Honoraria. White:Celgene: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Janssen: Consultancy, Honoraria. Reece:Takeda: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; BMS: Research Funding; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Membership on an entity's Board of Directors or advisory committees, Research Funding; Otsuka: Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Research Funding. Chen:Celgene: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Amgen: Honoraria. Louzada:Celgene: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Bayer: Honoraria. McCurdy:Janssen: Honoraria; Celgene: Honoraria. Hay:Janssen: Research Funding; Novartis: Research Funding; AbbVie: Research Funding; Kite: Research Funding; Takeda: Research Funding; Roche: Research Funding; Celgene: Research Funding; Seattle Genetics: Research Funding; MorphoSys: Research Funding; Gilead: Research Funding.
While Carfilzomib is approved for use in relapsed and refractory myeloma the combination with cyclophosphamide is not approved.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal