

Background: After long-term treatment with tyrosine kinase inhibitors (TKIs), an important proportion of patients with chronic myeloid leukemia (CML) achieve and maintain a deep molecular response (DMR) that allows them to stop treatment indefinitely. However, approximately 50% of these patients on treatment-free remission (TFR) experience relapse by undetermined reasons. It has been described that TKIs may induce a potent antileukemic response that conditions the outcome of the discontinuation. Our objective was to analyze different immune parameters that could be used as biomarkers of safer treatment discontinuation.
Objectives: To determine the modulation of immune biomarkers that could be related to current treatment with TKIs on patients with CML ("On TKI") or to successful TFR in patients that maintain DMR after treatment withdrawal ("Off TKI") or to relapse after TFR on patients that lost DMR.
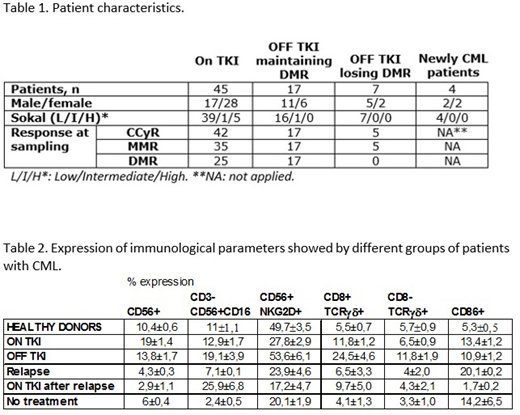
Materials & methods: We analyzed by flow cytometry the peripheral blood mononuclear cells (PBMCs) from 45 patients with CML "On TKI" for at least 9 months (imatinib (11), nilotinib (9), dasatinib (20) or bosutinib (5)), 17 patients "Off TKI" for at least 7 months who kept DMR at the moment of sampling (last TKI before TFR: imatinib (7), nilotinib (6), dasatinib(4)), 7 patients "Off TKI" for at least 1 year and 4 months who relapsed during TFR (samples from 3 patients were taken previous to TKI reintroduction (on relapse); samples from 4 patients were taken after they restarted treatment with TKIs ("On TKI" relapse), 4 patients with recent diagnosis of CML still untreated, and 20 healthy donors as basal control.
Results:
1) Patients characteristics are shown in table 1.
2) Treatment with TKIs induced an increase of 8.6±1.2% ((p<0.001) in CD56+ Natural Killer (NK) cells regarding healthy controls. This increase was sustained in patients "Off TKI" during successful TFR but it was reduced 9.5±1.4% in patients "Off TKI" on relapsed CML. This cell population was not recovered in patients on relapse even after restarting TKI treatment. 3) A population of NK cells with cytotoxic phenotype CD3-CD56+CD16+ was increased 8.1±2.8% in "Off TKI" patients during TFM, regarding patients on treatment. This population was reduced 12±3.8% in patients "Off TKI" who relapsed CML but increased 18.8±6.7% once treatment was restarted. 4) The expression of NKG2D - a major recognition receptor for the detection and elimination of cancerous cells - in NK cells was reduced 29.7±1.5% in patients "Off TKI" who relapsed during TFR, regarding "Off TKI" patients who kept DMR. This cell population was not recovered in patients on relapse even after restarting TKI treatment. 5) Populations of cytotoxic cells CD8+TCRgd+ and CD8-TCRgd+ were respectively increased 19±3.9% (p<0.0001) and 6.1±1.0% (p<0.05) in "Off TKI" patients regarding healthy controls but they were reduced 17.95±1.3% and 7.8±0.1%, respectively, in "Off TKI" patients who relapsed CML. 6) Expression of CD86, which has been related to poor prognosis, was increased 9.2±1.0% in patients "Off TKI" with relapsed CML, regarding to patients who maintained DMR on TFR.
Conclusions: Characterization of the immune response developed in patients with CML due to treatment with different TKIs may be relevant to predict the success of treatment discontinuation. We have determined that the modulation of the expression of the following markers may be used as potential predictors of TFR outcome: CD56+<4%; CD3-CD56+CD16+>7%; CD56+NKG2D+>24%; CD8+TCRgd+>7%; CD8-TCRgd+>4%; CD86+<20%. These biomarkers need to be validated in a larger cohort of patients.
This work was supported by NIH grant R01AI143567 and the Spanish Ministry of Economy and Competitiveness SAF2016-78480-R.
Garcia-Gutiérrez:Novartis: Honoraria, Other: Advisory Committees. Piris-Villaespesa:Novartis: Honoraria, Other: Advisory Boards.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal