

Introduction
The treatment landscape of Hodgkin Lymphoma (HL) has undergone a revolution in recent years, providing multiple options for providers and patients in their shared goal for disease control. However, these successful treatment options (e.g. multi-agent chemotherapy, radiotherapy, or combined modality) come at a high cost in the form of late effects, with little known about long-term toxicity of novel agents (e.g., Brentuximab vedotin, immunotherapy). As part of an international effort to develop tools to enhance treatment decision-making for providers and patients, we developed a survey to learn about what role HL survivors played in their initial treatment decision(s) as well as to understand survivors' knowledge and experience of late effects.
Methods
The survey titled Understanding of Decision-Making among HL Survivors included three themes: 1) initial treatment plan; 2) role in decision-making about the plan and factors important to the treatment selection; and 3) understanding of late effects. The survey was initially piloted at a cancer conference in Spring 2019 after which modest revisions were made to improve clarity. The revised survey was then distributed nationally in a single push through the Leukemia & Lymphoma Society's voluntary email listserv (Summer 2019). Responses were captured in the HIPAA complaint, web-based application, REDCap®, and then analyzed with descriptive statistics.
Results
A total of 129 HL survivors responded to the survey. The majority of respondents (n=98, 76%) identified as female. While nearly half (46%) were between 1-5 years from treatment, 27% were <1 year off therapy or still in treatment, and 27% were treated > 5 years ago. Age distribution at diagnosis ranged from <18 years (n=3, 2%), 18-25 years (n=35, 27%), and >26 years (n=91, 71%). Two-thirds (n=83, 64%) of patients were treated with chemotherapy alone. Overall, 90% of survivors reported receiving ABVD or a close variant (e.g., AVD).
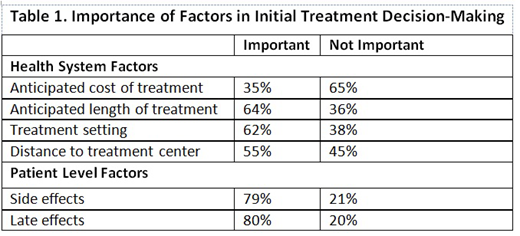
The majority of survivors (n=88, 68%) reported only receiving one treatment option by their oncologist. Half (n=69, 54%) engaged in shared decision-making with their physician, with or without family/friends, 24% (n=31) deferred to their physician, 20% (n=26) decided on their own or with family/friend, and 2% (n=3) followed the plan determined by their physician and family on their behalf. Most respondents were treated in the community (n=77, 60%) with an additional 34% (n=44) reporting having been treated at an academic medical center. For 8 respondents (6%) the treatment site was categorized as other. Survivors were asked to rate the importance of factors in their initial treatment decision-making on a 3-point scale. Results were then dichotomized to important or not important. Health systems factors (e.g., cost, distance) were deemed less important, while patient-level factors (e.g., side effects, late effects) were widely endorsed (Table 1).
The majority of survivors (n=107, 83%) were aware they are/may be at risk for late effects. Seventy percent (n=68 of 97) had been told at the time of discussion of treatment option(s) with their oncologist. The remainder (n=29 of 97, 30%) learned after completion of treatment or when transitioning care from their treating oncologist to survivorship or primary care. One third of respondents (n=46, 36%) reported they have been diagnosed with a late effect, which included substantial late effects of secondary malignancy (n=5, 11%) and cardiac toxicity (n=4, 9%).
Discussion
We report the results of a recent national survey of HL survivors, represented by an activated cohort that elects to participate in cancer advocacy groups. While two-thirds of respondents had little choice in initial treatment options, the majority endorsed the importance of side effects and late effects in treatment selection. Only half of survivors engaged in shared decision-making with their physician, indicating ample room for improvement and the development of tools to facilitate this process.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal