

Introduction
Doxorubicin carries a risk of heart failure (HF). Black race has been suggested as a risk factor for doxorubicin-related HF or asymptomatic LVEF decline, but studies were limited by small sample size, unknown racial composition of the comparison group, or lack of assessment of potential confounders. We aimed to assess whether HF occurs at higher rates in black patients (pts) compared to non-Hispanic white pts who receive doxorubicin for DLBCL, and to evaluate race as an independent risk factor for the development of HF after adjusting for known risk factors.
Methods
We used the Surveillance, Epidemiology, End Results - Medicare (SEER-Medicare) database to identify pts >65 years who were diagnosed with DLBCL (ICD-O: 9680, 9684) between 1997-2015 and who received doxorubicin (HCPCS/NDC codes) within 30 days of diagnosis. We excluded pts with HF (ICD-9: 428, ICD-10: I50) documented prior to diagnosis with DLBCL. We recorded age at diagnosis, Ann Arbor stage, and race. We assessed pts for hypertension (HTN) and coronary artery disease (CAD) documented in the year prior to lymphoma diagnosis. The primary outcome was documented HF at any point following DLBCL diagnosis.
Descriptive statistics were performed for demographic and clinical variables. The proportion of pts who developed HF was calculated in both racial groups and compared with the chi-square test. A multivariable logistic regression model was formulated using race, age at diagnosis, Ann Arbor stage and comorbidities, as covariates. Adjusted odds ratios and 95% confidence intervals for racial group status and demographic/clinical variables of interest were estimated from the multivariable model. The Kaplan-Meier method was used to generate time-to-event curves for the onset of HF in each racial group. A multivariable Cox proportional hazards model was used to estimate the hazard ratio for the diagnosis of HF in black vs. white pts after adjusting for age at diagnosis, stage, HTN and CAD. All p-values were two-sided with statistical significance evaluated at the 0.05 alpha level.
Results
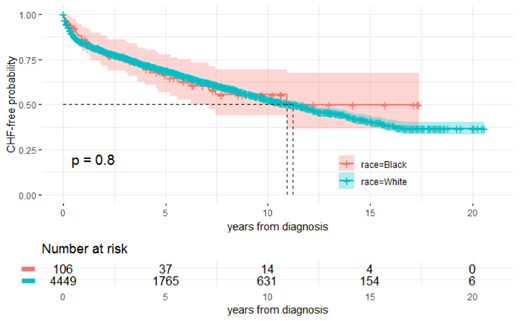
We identified 71,072 pts with DLBCL (white 82.2%, black 5.7%). We excluded 13,651 (19%) pts with HF prior to lymphoma diagnosis (white 84.4%, black 5.7%). We identified 6630 pts (white 88.8%, black 3%) with DLBCL who had received doxorubicin within 30 days of diagnosis. We excluded 797 pts <65 years and 802 pts with unknown stage at diagnosis. Of the remaining 4555 pts (white 97.7%, black 2.3%), 3398 (74.6%) had a history of HTN (white 74.3%, black 88.7%) and 1841 (40.4%) had a history of CAD (white 40.5%, black 37.7%). A total of 1607 (35%) pts developed HF (white 35%, black 33%). By univariate analysis, factors associated with development of HF included history of HTN (OR 1.27; 95% CI 1.10-1.47; p=0.001), CAD (OR 1.39; 95% CI 1.23-1.57); p<0.001), age at diagnosis of DLCBL (median 72.5 vs. 74; p=<0.001) and stage (OR 0.87; 95% CI 0.77-0.98; p=0.02). Race was not associated with risk of HF (OR 1.11; 95% CI 0.74-1.68; p=0.70). Our multivariable logistic regression model showed that older age at diagnosis (OR 1.03; 95% CI 1.02-1.04) and CAD (OR, 1.28; 95% CI 1.12-1.46) were associated with HF. Stage III/IV (OR 0.86; 95% CI 0.76-0.97) was associated with a lower risk of HF compared to stage I/II. Race (OR 1.05; 95% CI 0.70-1.60) and prior history of HTN (OR 1.12; 95% CI 0.96-1.30) were not significantly associated with development of HF. The median overall CHF-free survival time was 10.28 years after diagnosis (95% CI 9.75-11.13; Figure 1). Log-rank testing showed no difference in probability of developing HF between black and white pts (p=0.80), and the Cox model showed that after accounting for age at diagnosis, stage, HTN, and CAD, there was no statistically significant association between race and HF (HR, 0.92; 95% CI 0.66-1.30; p=0.62).
Discussion
HF is a common condition in older individuals following use of anthracycline for DLBCL, and it is associated with worse survival. No association was observed between black race and the onset of heart failure following treatment with doxorubicin for DLBCL. However, there was a greater proportion of black pts excluded for pre-existing HF than in the final study population. This highlights the importance of rigorous screening for pre-existing HF or LV dysfunction as a means of mitigating the risk of worsening cardiac function in this population.
Martin:I-MAB: Consultancy; Sandoz: Consultancy; Karyopharm: Consultancy; Teneobio: Consultancy; Celgene: Consultancy; Janssen: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal